Why Do So Call Health Conscious People who go to Gym Daily and Do Proper Exercises Get Heart Attack and that too at younger Age ?
Should we go to Gym or Not ?
Let us see
-oOo-
Consciousness and Awareness have different meanings when used as Adjective
For example
Health Conscious – Means Knowing the importance of maintaining Good Health and doing somethingfor that
Health Awareness – Means Means Knowing the importance of maintaining Good Health and doing the right thingfor it
-oOo-
Those who don’t mind about the health are not health conscious. Examples are those who don’t know what is their Blood Sugar and Blood Pressure
Those who mind about their health, but do the wrong things are health-conscious, but not health-aware. These are people who know about diabetes, have checked their blood sugar and found that they have diabetes, but read “Organic Eugenics” books and watch such videos and eat millets and jaggery and pay lots of money for “Chekku” Oil
Those who mind about their health, but do the correct things are health-conscious as well as health-aware. These are people who know about diabetes, have checked their blood sugar and follow scientific methods to improve their health
-oOo-
The common factor behind diseases like Heart Attack, Stroke, Vision Problems, Kidney Failure etc is clogging of blood vessels.
This clogging of blood vessels is due to
(I)
Damage to the inner wall of the blood vessels. (Scientifically it is called Endothelial Damage)
(II)
Increased Clot Forming Ability
-oOo-
(I)
This damage to the inner wall happens because of various reasons
(I.A) Structurally Weak Inner Wall
1. Those whose inner wall is weak due to various Genes. In these people, even a normal blood sugar and normal blood pressure cause more damage
(I.B) Damage Due to Mechanical Reasons
2. High Blood Pressure. Your Blood Vessels are like Pipes or Garden Hoses. What happens when the pressure of water flowing in a pipe is high. It gets damaged easily. Isn’t it. Similarly when the blood pressure is high, your blood vessel’s inner wall get damaged soon.
3. High Pulse Rate : What happens when you take a straw and fold it. You will see a damage in the straw. What if you fold again and again. At one point the damage will be severe. Same way, When your blood vessels are bent and unbent again and again, the rate of injury to the inner walls. There are many blood vessels which get bent again and again. The vessels which gets bent maximum times in the one in your heart. It gets bent every time your heart beats. The vessels of your neck gets bent every time you move your neck. The vessels of your knee gets bend every time you move your knee. (This is why atherosclerosis is so common in Coronary, Carotid, Vertebral and Popliteal arteries)
(I.C) Damage Due to Chemical Reasons
Assume few different garden hoses. One in which only water flows. Another in which acid flows. Which will get damaged quicker ?
Same way,
Your blood vessels are also damaged as per what is in the blood
4. High Blood Sugar : Damages the blood vessels and leads to reduced blood flow. This is exactly why we need to keep the blood sugar under control. The damages may not be visible immediately, but they will accumulate
5. High LDL : Just like High Cholesterol, this too damage the blood vessels
6. Free Radicals : also damage the inner wall
7. Hyperhomocysteinemia : Homocysteine is a sulfur amino acid whose metabolism stands at the intersection of two pathways: remethylation to methionine, which requires folate and vitamin B12 (or betaine in an alternative reaction); and transsulfuration to cystathionine, which requires pyridoxal-5′-phosphate. When there is problem in either of these pathways, the level of Homocysteine in the body increases. When it increases beyond a certain level, it causes damages to the inner wall of the blood vessels causing reduction in blood flow.
(II) Increased Clot Forming Ability : Hope you know the disease Hemophilia. This is a condition where blood does not clot easily. There are lots of diseases where the other end happens. That is Blood clots easily. In such cases, the person is at risk of developing clot even when Blood Sugar, Pressure, Cholesterol levels are normal. And the most important part is these conditions cannot be solved by exercise, walking etc
Increased Clot Forming Ability can be due to
(II.A) Congenital / Inborn : These are due to reasons where the individual has few genes which increase the clot forming ability of blood
8. Factor V Leiden and Prothrombin G2021A mutation.
9. Antithrombin III, protein C and protein S deficiency
So
Whether you will get a heart attack (or stroke or kidney failure or vision problem or neuropathy) depends on so many factors
And
You need evaluate and manage accordingly
-oOo-
So
1. You get heart attack if your vessels are weak from birth due to your genes
2. You get heart attack if your BP is high
3. You get heart attack if your Pulse is high
4. You get heart attack if your blood sugar is high
5. You get heart attack if your LDL is high (please don’t get fooled by half baked idiots who say that LDL is not an issue)
6. You get heart attack if Free Radicals are high in your body
7. You get heart attack if there is homocysteinaemia
8. You get heart attack if you have Factor V Leiden and Prothrombin G2021A mutation. (Please don’t order a test yourself and spend 1000s of rupees and then go an ask the doctor to explain it. It does not work that way)
9. You get heart attack if you have Antithrombin III, protein C and protein S deficiency
10. You get heart attack if you undergo Surgery,
11. You get heart attack if you are Pregnant and have other heart issues
12. You get heart attack if you undergo Hormonal replacement therapy,
13. You get heart attack if you use Hormonal Contraception (Condoms are the safest)
14. You get heart attack if you have cancer (malignancy)
15. You get heart attack if you have Inflammation,
16. You get heart attack during or after Infection eg Post COVID 19 Thrombosis
-oOo-
So there are multiple factors
I have listed just a few
There are many others too
-oOo-
So Treatment to prevent Heart Attack (or other such complications) has to be a multi pronged approach.
Exercise and Diet are the first line of approach But at the same time, you need to understand that mere Exercise won’t help and Mere Diet won’t help
-oOo-
Now
What will happen when a person exercises
Heart Rate will increase
BP will increase
What happens when heart rate increases
There is bending and unbending the the blood vessels of heart
What happens when BP increases
There is increased pressure to the inner wall of the blood vessels of heart
What happens when there is bending and unbending and increased pressure There is damage to the inner wall
-oOo-
Now Coming to the Questions
Why Do So Call Health Conscious People who go to Gym Daily and Do Proper Exercises Get Heart Attack and that too at younger Age ?
When you exercise, you damage your inner wall. Now, if there are no other causes for damage to wall and if there are no other causes of increased coagulability at work, there is time for the damages to be repaired
But
When other risk factors (increased sugar, increased LDL, post covid thrombosis) are also present There is no time for the body to repair the damaged inner walls and there is an heart attack
-oOo-
Should we go to Gym or Not ?
Please go to Gym
But Please correct your Blood Sugar, Pulse Rate, Blood Pressure, Hypercoagulability first and then go to Gym
-oOo-
If you have no risk factors –> Gym increases your lifespan
If you have risk factors and have corrected them with diet + drugs –> Gym increases your lifespan
If you have risk factors and you have avoided tablets and think that you can solve all the problems with exercise alone –> Gym REDUCES your lifespan
-oOo-
Moral
1.
Human Body Structures are complex
Human Body Functions are complex
There are multiple factors at play
2.
Don’t follow some advice based on Whatsapp forwards / Facebook Posts / Videos / Instagram Reels. Many of such Videos (including the one by few “doctors” are based on some random articles with scant regard to Physiology, Pathology, Community Health).
3.
When you have risk factors, Tablets plus Gym is Best
When you have risk factors, Tablets alone are better
When you have risk factors, Keeping Quite and Doing nothing is bad
When you have risk factors, Gym without Tablets is giving Friend Request to EmaDharmaRaja and then calling him over phone and asking to accept the request !
-oOo-
Feel free to ask doubts
If you want to know about complications of diabetes and how to prevent them, read this book : Myths and Facts about LCHF (Low Carb High Fat) Diet and “Reversal” of Type 2 Diabetes: How Paleo, Keto, Atkin’s Diets Work https://amzn.to/3VbRcac
Myths and Facts about LCHF (Low Carb High Fat) Diet and “Reversal” of Type 2 Diabetes: How Paleo, Keto, Atkin’s Diets Work
நீரழிவு நோய்க்கு ஏற்ற உணவு குறித்து அறிய : பேலியோ உணவின் அறிவியலும் உளவியலும்: Science and Psychology of Paleo Diet (Tamil Edition) https://amzn.to/3XcZSPw நூலை வாசிக்கவும்
புருனோ Bruno பேலியோ உணவின் அறிவியலும் உளவியலும்: Science and Psychology of Paleo Diet
கிணற்றில் இருந்து நீரை எடுக்கவேண்டுமென்றால் கயிற்றில் வாளியை கட்டி எடுக்கலாம்.
அல்லது ஓடி (மோட்டார்) மூலம் எடுக்கலாம். அப்படி ஓடி (மோட்டார்) மூலம் எடுக்கும் போது நீர் வர ஒரு குழாய் தேவை. அத்துடன் ஓடிக்கு மின்சாரம் கொண்டு வர கம்பி (வயர்) தேவை
-oOo-
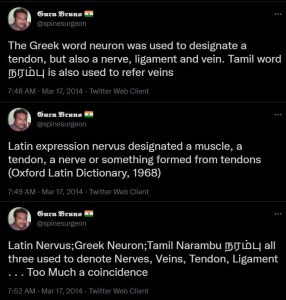
Bruno’s Tweet on Nerve Vein Artery
இதே போல் நமது உடம்பில் சில உறுப்புகள் உள்ளன. எலும்புகளை எலும்புடன் சேர்க்கும் எலும்புநாண் / எலும்புநார் (Ligament)
எலும்புகளை தசையுடன் சேர்க்கும் தசைநார் (Tendon)
இரத்தத்தை கொண்டு சேர்க்கும் இரத்தக்குழாய்கள் (Blood Vessels)
உறுப்புகளில் இருந்து மூளைக்கு செய்திகளை அனுப்பும், மூளையில் இருந்து உறுப்புகளுக்கு செய்திகளை அனுப்பு நரம்புகள் (Nerves)
-oOo-
இதில் இரத்த குழாய்கள் என்பது இருவகைப்படும்
இதயத்தில் இருந்து பிற உறுப்புகளுக்கு இரத்தத்தை கொண்டு செல்லும் தமணிகள் (Arteries)
பிற உறுப்புகளில் இருந்து இதயத்திற்கு இரத்தத்தை கொண்டு செல்லும் சிரைகள் (Veins)
-oOo-
உடலில் நீர்ச்சத்து குறைவாக இருந்தால் நாம் திரவங்களை ஏற்றுகிறோம் அல்லவா. அதற்கு நாம் பயன்படுத்துவது சிரைகளை (Veins). இரத்தம் ஏற்ற வேண்டும் என்றாலும் சிரைகள் மூலம் தான் ஏற்றவேண்டும். அதே போல் ஊசியில் மருந்து செலுத்தும் போதும் சிரைகளில் செலுத்தலாம். இதை சிரை வழி திரவம், (Intravenous Infusion) சிரை வழி ஊசி / சிரையுள் ஊசி, சிரைவழியாக ஊசி, சிரையக ஊசி (Intravenous Injection or IV Injection) என்று அழைப்பார்கள்.
தசைகளில் (தோளில், பிட்டத்தில்) போடப்படும் ஊசி தசையுள் ஊசி (Intra muscular Injection or IM Injection).
தோலுக்கு அடியில் போடப்படும் தோலடி ஊசி (Subcutaneous Injection or SC Injection)
தோலுக்குள் போடப்படும் ஊசியும் உண்டு (Intradermal)
-oOo-
இன்று நாம்
எலும்புநாண் / எலும்புநார்
தசைநாண் / தசைநார்
தமணி
சிரை
நரம்பு
என்று பிரித்து சொன்னாலும்
ஒரு காலத்தில்
இவை அனைத்தையும் நரம்பு என்றே அழைத்தார்கள்.
இந்த பிரச்சனை தமிழில் மட்டுமல்ல, கிரேக்க மொழியிலும், இலத்தீன் மொழியிலும் இதே போல் தான் இருந்துள்ளது
The Greek word neuron was used to designate a tendon, but also a nerve, ligament and vein.
Latin expression nervus designated a muscle, a tendon, a nerve or something formed from tendons (Oxford Latin Dictionary, 1968)
Latin Nervus; Greek Neuron; Tamil Narambu நரம்பு all three used to denote Nerves, Veins, Tendon, Ligament
-oOo-
எனவே சிரைவழி ஊசிகளை நம் மக்கள் நரம்பூசி என்றே அழைத்தனர்.
முன்னோர் தான் முட்டாள் இல்லையே, பிறகு நாம் ஏன் அதை மாற்றவேண்டும், அப்படியே தொடர்ந்து அழைக்கக்கூடாது என்று கேள்வி எழுகிறதா ?
இதற்கு பதில் உள்ளது
சுமார் 100 ஆண்டுகளுக்கு முன்னர் சிரை வழி ஊசிகள் மட்டுமே போடப்பட்டு வந்தன. எனவே நரம்பூசி என்று அழைத்தாலும் கூட அது சிரைக்குள் செலுத்துவதை மட்டுமே குறித்தது.
ஆனால்
அறிவியல் வளர வளர
தமணிக்குள்ளும் ஊசிகளை செலுத்தும் பழக்கம் வந்தது. முக்கியமாக புற்று நோய் சிகிச்சையில் இது 1950களில் இருந்தே பயன்பாட்டில் உள்ளது (Klopp CT, Alford TC, Bateman J, Berry GN, Winship T. Fractionated intra-arterial cancer; chemotherapy with methyl bis amine hydrochloride; a preliminary report. Ann Surg. 1950;132:811–32 & Bonner CD, Thurman A, Homburger F. A critical study of regional intra-arterial nitrogen mustard therapy in cancer. Ann Surg. 1952;136:912–8)
அதே போல்
நரம்புகளை சுற்றி மருந்து செலுத்தும் பழக்கமும் உள்ளது. அறுவை சிகிச்சையின் போது வலி தெரியாமல் இருக்க போடுகிறார்கள் அல்லவா. அந்த ஊசியை நரம்புகளை சுற்றி செலுத்துவார்கள். இதை மரத்து போகும் ஊசி என்றும் அழைப்பார்கள். ஸ்பைனல் அனஸ்தீசியா என்பதும் இந்த வகைதான்
எனவே இன்றைய தேதியில்
நரம்பூசி என்பது வேறு
தமணியுள் ஊசி என்பது வேறு
சிரையுள் ஊசி என்பது வேறு
எனவே
இனியும் சிரைவழி திரவங்களையும், சிரையுள் ஊசியையும் “நரம்பூசி” என்று பொதுவாக அழைப்பதை தவிர்க்கலாமே
-oOo-
நரம்பு துண்டாகி இரத்தப்போக்கு ஏற்பட்டு வாலிபர் பலி என்று இந்த செய்தியில் தவறாக உள்ளது
நரம்பு துண்டாகி இரத்தப்போக்கு ஏற்பட்டு வாலிபர் பலி என்று இந்த செய்தியில் தவறாக உள்ளது
தமணி துண்டாகி அல்லது சிரை துண்டாகி என்று எழுதியிருக்கவேண்டும். தமணியா, சிரையா, எது பிரச்சனை என்று தெரியாவிட்டால் ”இரத்தக்குழாய் துண்டாகி என்று எழுதியிருக்கலாம்” இப்படி எழுதுவது பிழை
ஒருவருக்கு பைல்ஸ் பிரச்சனை அல்லது சிறுநீரக கோளாறு இருக்கிறது என்று வைத்துக்கொள்ளுங்கள்.
இப்பொழுது அவர் வைத்தியம் செய்து கொள்ள நிறைய இடங்கள் உள்ளன
1. அரசு மருத்துவமனையில் – இலவசமாக
2. தனியார் மருத்துவமனையில் – காசு கட்டி
3. தனியார் மருத்துவமனையில் – காப்பீடு மூலம் (அதாவது ஏற்கனவே காப்பீடு திட்டத்தில் சேர்ந்திருந்தால்)
எந்த மருத்துவமனை செல்வது என்பதை தீர்மானிக்க அவருக்கும் அவரது குடும்பத்தினருக்கும் நேரம் உள்ளது.
அவர் தனியார் மருத்துவமனையில் சேர்கிறார் என்றால், அவர் பணம் கட்டுவார் அல்லது அவரது காப்பீடு திட்டத்தை வைத்து அந்த மருத்துவமனை காப்பீடு நிறுவனத்திற்கு விண்ணப்பிப்பார்கள். அப்படி விண்ணப்பித்தவுடன், அந்த நிறுவனம் அதை அங்கீகரிக்கும். அதை வைத்து சிகிச்சை துவங்கும்
அவசரமில்லாத சிகிச்சைகளுக்கு இந்த பிரச்சனை இல்லை ஆனால் விபத்துக்களில் சிக்கல் உள்ளது
-oOo-
அடி சிறிது என்றால் – சிராய்ப்பு மட்டும் தான் என்றால்- முதலுதவி சிறிது தான், சிகிச்சையும் சிறிது தான்.
ஆனால் அடி பலம் என்றால் – தலைக்காயம் அல்லது விலா எலும்பு முறிவு, கை கால் எலும்பு முறிவு என்றால்- முதலுதவியும் அதிகம், சிகிச்சையும் அதிகம்.
உதாரணமாக,
சிராய்ப்பு என்றால் முதலுதவிக்கு 100 ரூபாய் ஆகும். மொத்த வைத்தியம் ரூ500 முதல் ரூ1000 வரை ஆகும்.
கை எலும்பு முறிவு என்றால் முதலுதவிக்கு 1000 ரூபாய் ஆகும். மொத்த வைத்தியம் ரூ10000-ரூ30000 வரை ஆகலாம்.
கால் எலும்பு முறிவு என்றால் முதலுதவிக்கு 10000 ரூபாய் ஆகும். மொத்த வைத்தியம் ரூ1 லட்சம் – ரூ2 லட்சம் வரை ஆகலாம்.
தலைக்காயம் / முதுகு எலும்பு முறிவு என்றால் முதலுதவிக்கே ரூ1 லட்சம் ஆகும். மொத்த கட்டணம் ரூ3 லட்சம் முதல் ரூ10 லட்சம் ஆகலாம்
இது புரிந்து கொள்ளத்தான். சரியான கட்டணம் என்பது நபருக்கு நபர் மாறுபடும்.
-oOo-
முதலுதவிக்கு 1 லட்சமா என்று கேள்வி எழுகிறதா ?
1980களில் முதலுதவி என்பது கட்டு போடுவது + வலிக்கு மாத்திரை அளிப்பது மட்டுமே. 1980களில் முதலுதவி என்பதை ஒரு சிறிய பெட்டிக்குள் அடக்கி விடலாம்
2021ல் முதலுதவி என்பதே பெரிதாகிவிட்டது
Philadelphia Collar / Spine Board / Pelvic Binders / Splints
Suction / OP Airway / NP Airway / Intubation / Tracheostomy
Ventilatory Suppor
Venflon / Central Line
Stat Lab
Volume Replacement Blood Transfusion
X Ray / eFast / CT / MRI
ICD / Pericardiocentesis
எனவே இன்றைய தேதிக்கு
உண்மையான முதலுதவி என்பது விபத்தின் தன்மையை பொருத்து 10 ரூபாயில் இருந்து (சிராய்ப்பு என்றால்) ரூ1 லட்சம் வரை (தலைக்காயம் + எலும்பு முறிவு + நுரையீரல் பாதிப்பு) ஆகும்.
-oOo-
சும்மா ஒரு கட்டு போட்டுவிட்டு, டிடி ஊசி போடுவது என்றால் 100 ரூபாய் செலவு. ஆனால் உண்மையில் உயிரை காக்க வேண்டும் என்றால் 1 லட்சம் செலவு.
சும்மா ஒரு கட்டு போட்டுவிட்டு, டிடி ஊசி போடுவது என்றால் 10 நிமிடம் தான் ஆகும். ஆனால் உண்மையில் உயிரை காக்க வேண்டும் என்றால் 6 மணி நேரம் வரை ஆகலாம்.
-oOo-
அந்த காலத்தில் எல்லாம் அடிபட்டால் 10 ரூபாய் தான் செலவு. இப்ப 1 லட்சமா, ஹாஸ்பிட்டல் எல்லாம் கொள்ளையடிக்கிறாங்க என்று புலம்புகிறீர்களா ?
சற்றுப் பொறுங்கள்.
விபத்தினால் நேரும் மரணங்களை கீழ்க்கண்டவாறு பகுக்கலாம்.
(1) முதல் வகை: மூளை, இதயம், மகாதமணி, முதுகுத்தண்டு ஆகியவை கிழிபடுவதால் ஏற்படும் உடனடி மரணம் – இது அடிபட்ட சில நொடிகளில் இருந்து 10 நிமிடங்களுக்குள் ஏற்படும். இதில் உயிரை காக்க வாய்ப்பு குறைவு. விபத்தை தடுப்பதன் மூலமே இதை தடுக்க முடியும்.
(2) இரண்டாம் வகை : மண்டக்குள் இரத்தக்கட்டு, நுரையீரலை சுற்றி இரத்தம் கட்டுவது, இதயத்தை சுற்றி இரத்தம் கட்டுவது, இரத்தப்போக்கு, மூச்சுத் திணறல் ஆகியவற்றால் ஏற்படும் மரணங்கள். இவை 10 நிமிடங்களில் இருந்து 2-3 நாட்களுக்குள் ஏற்படும். ஆனால் அடிபட்ட உடனே, அடிபட்ட 1 மணி நேரத்திற்குள் சிகிச்சையை அளிப்பதன் மூலம் இவர்களின் உயிரை காக்க முடியும்.
(3) மூன்றால் வகை : பிற அடிகள்.
-oOo-
1980களில் முதலுதவி என்பது கட்டு போடுவது + வலிக்கு மாத்திரை அளிப்பது மட்டுமே. 1980களில் முதலுதவி என்பதை ஒரு சிறிய பெட்டிக்குள் அடக்கி விடலாம். காரணம் அன்றைய காலக்கட்டத்தில் நாம் மூன்றாம் வகை அடிகளுக்கு மட்டும் தான் முதலுதவி செய்து வந்தோம்.
அன்றைய காலக்கட்டத்தில்
மண்டைக்குள் இரத்தக்கட்டு, நுரையீரலை சுற்றி இரத்தம் கட்டுவது, இதயத்தை சுற்றி இரத்தம் கட்டுவது, இரத்தப்போக்கு, மூச்சு திணறல் ஏற்பட்டால் மரணம் தான்.
அதாவது 1980களை பொருத்தவரை,
முதல் வகை + இரண்டாம் வகை இரண்டுமே ஸ்பாட் அவுட் தான்
ஆனால் 2021ல் நவீன அறிவியல் மருத்துவம் வளர்ந்த பிறகு இரண்டாம் வகைக்கு சிகிச்சை வந்துள்ளது. அதன் மூலம் உயிரை காக்க முடிகிறது. ஆனால் இதற்கு ரூ3 லட்சம் முதல் 10 லட்சம் வரை ஆகிறது. இந்த முதலுதவிக்கே ரூ1 லட்சம் ஆகிறது
அந்த காலத்தில் அடி பட்டு “ஸ்பாட் அவுட்” என்று கணக்கில் வந்தவர்களில் பாதி பேரை காக்க முதலுதவிக்கே 1 லட்சம் ஆகிறது.
அதாவது 10 ரூபாய் கட்டு போதுவது 1 லட்சம் ஆகவில்லை, புதிதாக 1 லட்சத்திற்கு சிகிச்சை வந்துள்ளது.
-oOo-
ஒருவர் சாலையில் செல்லும் போது விபத்துக்காகிறார் என்றால், அவர் கையில் 1 லட்சம் இருந்தால் அவருக்கு தனியார் மருத்துவமனையில் சிகிச்சை அளிப்பதில் எந்த பிரச்சனையும் இல்லை.
அவர் கையில் காசு இல்லை என்றால் அந்த தனியார் மருத்துவமனைக்கு யார் காசு கொடுப்பார்கள்?
அவர் கையில் காசு இல்லை, ஆனால் அவரிடம் காப்பீடு உள்ளது. அந்த காப்பீடு எண் கையில் இல்லை. அந்த தனியார் மருத்துவமனைக்கு யார் காசு கொடுப்பார்கள்?
இது தான் இன்று வரை இருந்த நடைமுறைச் சிக்கல்.
-oOo-
உதாரணமாக
ஒருவருக்கு விபத்தில் கை எலும்பு முறிந்துள்ளது, இது வரை 108 அம்புலன்ஸ்
அவரிடம் பணம் இருக்கிறதா?, காப்பீடு உள்ளதா?, உறவினர்களால் பணம் செலுத்த முடியுமா? என்ற எந்த கேள்வியும் கேட்காமல்
அவரை அரசு மருத்துவமனைக்குத்தான் அழைத்து செல்லும். அங்கு சென்று அவருக்கு முதலுதவி செய்யப்படும்.
பிறகு உறவினர்கள் எல்லாம் வந்த பிறகு
1. அவர்களிடம் காசு இல்லை என்றால் அவர்கள் அரசு மருத்துவமனையில் சிகிச்சை தொடரலாம்.
2. அவர்களிடம் காசு அல்லது காப்பீடு இருந்தால் வேறு தனியார் மருத்துவமனை செல்லலாம்.
-oOo-
உதாரணமாக,
ஒருவருக்கு விபத்தில் கை எலும்பு முறிந்துள்ளது
அவரிடம் பணம் உள்ளது.
அவர் தனியார் மருத்துவமனை தான் செல்வேன் என்று சொன்னால் அம்புலன்ஸ் அவரை அங்கு அழைத்து செல்வார்கள்.
-oOo-
உதாரணமாக,
ஒருவருக்கு விபத்தில் தலையில் அடிபட்டு மயக்கமாகியுள்ளார். அவர் யார் என்றே தெரியாது. இது வரை 108 அம்புலன்ஸ்
அவரை அரசு மருத்துவமனைக்குத்தான் அழைத்து செல்லும். அங்கு சென்று அவருக்கு முதலுதவி செய்யப்படும்.
பிறகு உறவினர்கள் எல்லாம் வந்த பிறகு
1. அவர்களிடம் காசு இல்லை என்றால் அவர்கள் அரசு மருத்துவமனையில் சிகிச்சை தொடரலாம்.
2. அவர்களிடம் காசு அல்லது காப்பீடு இருந்தால் வேறு தனியார் மருத்துவமனை செல்லலாம்.
-oOo-
இப்பொழுது தமிழக அரசு கொண்டு வந்துள்ள திட்டம் என்ன?
முழுசிகிச்சையில் முதலுதவி பகுதியை மட்டும் தனியாக பிரித்து அந்த முதலுதவிக்கு தமிழக அரசு பணம் கொடுக்கும் என்பது தான்.
இந்த திட்டத்தின் மூலம்
விபத்தில் அடிபட்டவரை அரசு மருத்துவமனைக்குத்தான் கொண்டு வரவேண்டும் என்ற அவசியம் இல்லை.
அருகில் உள்ள தனியார் மருத்துவமனைக்கும் கொண்டு செல்லலாம். முதலுதவிக்கு அரசு பணம் கொடுக்கும் என்பதால்
மருத்துவமனையும் பணம் பற்றி கவலைப்படாமல் சிகிச்சையை துவங்குவார்கள். அவருக்கு முதலுதவி சீக்கிரம் கிடைக்கும்.
பிறகு அவரது உறவினர்கள் வந்த பிறகு அவர்கள் ஆற அமர முடிவு செய்து (இரண்டு நாட்களுக்குள்)
1. காசு அல்லது காப்பீடு இல்லை என்றால் அரசு மருத்துவமனைக்கு வரலாம்
2. காசு அல்லது காப்பீடு உள்ளது என்றால் அதே மருத்துவமனையில் தொடரலாம்
3. காசு அல்லது காப்பீடு உள்ளது என்றால் வேறு தனியார் மருத்துவமனை செல்லலாம்
-oOo-
இதனால் என்ன பலன்?
1. அடிபட்டவருக்கு : உதவி சீக்கிரம் கிடைக்கும். எனவே உயிரை காக்க வாய்ப்பு அதிகம். கை கால் ஆகியவற்றில் அடி பட்டிருந்தால் அந்த உறுப்புகளை காக்கவும் வாய்ப்பு அதிகம்.
2. உறவினர்களுக்கு : ஒருவர் விபத்தில் அடிபட்டார் என்பது அதிர்ச்சி தரும் செய்தி. அந்த நிலையில் அதே மருத்துவமனையில் தொடர்வதா, வேறு எங்கும் செல்வதா, எவ்வளவு காசு ஆகும், கையில் காசு உள்ளதா, கடன் வாங்குவதா, நகையை அடமானம் வைப்பதா என்ற முடிவு எடுக்கவேண்டாம்.
3. தனியார் மருத்துவமனைக்கு: அந்த நபர் அதே மருத்துவமனையில் சிகிச்சையை தொடர்ந்தால், அவர்களுக்கு வருமானம்.
4. அரசிற்கு : மக்களின் உயிரை காக்க முடியும்.
-oOo-
சும்மா இருப்பவர்களை கூட தனியார் மருத்துவமனைகள் பெரிய அடி இருப்பதாக காண்பித்து அதிக கட்டணம் வாங்க முடியுமா ?
முடியாது.
(1) 108 அம்புலன்ஸ்சில் ஒருவர் ஏறும் போதே அவரது உடல்நிலை என்ன என்பது குறித்து அவர்கள் பதிந்துவிடுவார்கள். அதை வைத்தே அவரின் முதலுதவிக்கு எவ்வளவு பணம் தேவை என்பதை சொல்லிவிடலாம்.
(2) விபத்து நடந்த பிறகு காவல் துறையினர் முதல் தகவல் அறிக்கை பதிவார்கள். அதிலும் காயங்களின் தன்மை இருக்கும்.
எனவே இந்த இரண்டையும் வைத்து
இது 100 ரூபாய் முதலுதவியா, (சிராய்ப்பா) 1000 ரூபாய் முதலுதவியா, (கை எலும்பு முறிவா) 10000 ரூபாய் முதலுதவியா, (தொடை எலும்பு முறிவா) அல்லது 1 லட்சம் முதலுதவியா (தலைக்காயம், வயிறு கிழிந்துவிடுவது) என்பதை எளிதில் கண்டு கொள்ளலாம்.
-oOo-
“காவல்துறையும் மருத்துவமனையும் சேர்ந்து ஊழல் செய்வார்கள், எனவே இந்த திட்டத்தை எதிர்க்கிறேன்” என்று கூறுகிறீர்கள் என்றால் avada kedavra என்பதை தவிர சொல்ல எதுவும் இல்லை.
மேலும் அறிந்து கொள்ள இந்த காணொளியை பார்க்கலாம்
மருத்துவம் தொடர்பாக மூத்த எலும்பியல் மருத்துவர் லோகநாதன் சார் அவர்களின் பிற காணொளிகளை இங்கு காணலாம்
IKT – 48 மணி நேரம் நம்மைக்காக்கும் இன்னுயிர் காப்போம் திட்டம்
Creating Emergency Care Fund (IKT Fund)
50 Cr Assurance Mode
Fix ceiling of up to Rs. 1 lakh per individual
Empanelment of Government and Private Hospitals – 609
Integrate the 48 hour cashless scheme with the existing CMCHIS scheme after 48 hours
Selection of 81 Appropriate Packages
IKT Empanelled 609 Hospitals
Government Hospitals
Private Hospitals
Level 1 Hospitals
20
30
50
Level 2 Hospitals
74
157
231
Level 3 Hospitals
121
207
328
215
394
609
The Scope of coverage
If a patient needs admission and minor procedure (listed) which does not exceed 48 hours stay the same may be done at the hospital he/she is being admitted.
If the patient is not stable or requires procedures that may need Hospitalisation beyond 48 hours one of the following conditions may apply.
Stabilization of the patient and Discharge to any empanelled Hospital if the patient needs further treatment which is covered under Chief Minister’s Comprehensive Health Insurance Scheme and is eligible for Coverage.
Stabilization of the patient and Discharge to Government Hospital if the patient needs further treatment but the treatment is not covered under Chief Minister’s Comprehensive Health Insurance Scheme or eligible for Coverage.
Stabilization of the patient and continuation of treatment in same Hospital or any other hospital of his / her choosing if the patient is not willing for transfer to Government Hospital (or) has private Insurance (or) willing to continue treatment as a paid patient.
IKT – Categories of patients who will benefit under NK – 48
All accident victims on road within TN border including tourists from other states and foreigners
Accident victims brought by Good Samaritans
Accident victims brought by family
Accident victims who come by themselves
Unknown accident victim brought by police, or Good Samaritans
Mass casualty accident victims
IKT – NK 48 Exclusion criteria
Assault injuries
Domestic injuries
Fall from height
Injuries due to fall of heavy object
Train traffic accident injuries
Animal bites, Self harm
Occupational work place injuries
Thermal /Chemical/ Burn Injuries
Cracker Blast Injuries
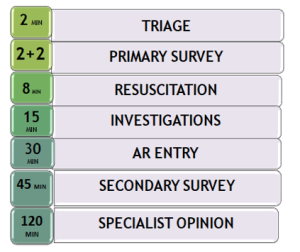
5 Steps of Emergency Trauma Care
Prehospital Triage & Transportation by Ambulance along with in-transit care
Resuscitation & Stabilization in hospital Emergency Department
Damage Control Surgeries
Definitive Care
Rehabilitation
Step 1,2,3 – IKT
Steps 4,5 – KKT – CMCHIS
NK 48 Guideline
On receipt of information from the accident site, Life support ambulance with trained manpower will reach the spot, Triaging & basic resuscitation (cABC) will be done by EMT.
Patients maybe entitled for free treatment upto 48 hours in hospitals of IK – NK 48 Scheme empanelled private hospitals of neighbouring states if the accident occurs within Tamil Nadu but close to the state border.
NK 48 Guideline
5 Levels of triaging at the Accident Scene for guiding the EMT
Pre-hospital Triage & Acuity Scale
Description of the Acuity Scale
Equivalent Triage category
Level 1 – Resuscitation
Patient battling for life in need of resuscitation/Severe hemodynamic compromise/Shock/Traumatic amputation of an extremity
Red
Level 2 – Emergent
Seriously injured patient who requires rapid medical intervention/Penetrating head,chest or abdominal injury/Neurovascular compromise of an extremity
Red
Level 3 – Urgent
Patient with stable vitals, but the presenting problem suggests further evaluation
Minor contusions, abrasions, lacerations not requiring closure, Non urgent with minor complaint
Green
RTA – Patient comes to any Hospital
IK NK 48 Basic Trauma Package for any RTA Patient – Clinical examination ,Hb, Urea, Sugar,ECG,X –Ray Chest. Patient is stable. He will be discharge (Green Category)
Patient in Red / Yellow category
CMCHIS Card Holder(Upto 48 hours) IK – NK48 Empaneled Hospital
Treatment under IK – NK 48 Packages
CMCHIS Non Card Holder / other state / Foreign RTA victims (Upto 48 hours) IK – NK48 Empaneled Hospital
Treatment under IK – NK48 Packages
Packages applicable only Upto 48 Hours in the NK 48 empanelled 609 hospitals only. IFT Can be done within 48 hours based on the triage only among the NK 48 empanelled 609 hospitals
Treatment will be continued under CMCHIS as per existing packages
Non CMCHIS Card holder ( Govt / Pvt empanelled Hospitals under CMCHIS)
Treatment will be continued under free category in Govt Hospitals
Treatment will be continued under payment / pvt insurance by the patient in pvt hospitals
Other state / foreign RTA victims
Treatment will be continued under free category in Govt Hospitals
Treatment will be continued under payment / pvt insurance / PM-JAY by the patient in pvt hospitals
NK 48 Guideline
Critically ill (Red category) patient to be taken by 108 Ambulance service to the nearest empanelled Level 1 Hospital if located within 20-30km.
The Level 1 Hospital may be a Government Hospital or a private facility.
The patient should be transported in the shortest period to ensure advanced trauma life support.
If it is far, the patient should be stabilized in the nearest L2 or L3 hospital and through 108 ambulance should move the patient after stabilization to the L1 facility for definitive intervention.
2 hr mandatory resuscitation for a critically injured patient before any Inter-facility Transfer.
IFT with Pre-Arrival Intimation to the receiving hospital.
Time Norms in Emergency Care of RTA patients
NK 48 Guideline – Preauth & Claim
EI number should be obtained by the treating hospital, & the URN should be shared even with IFT(Inter facility transfer) Hospital till the treatment course is completed under IKT.
When treatment involves more than 1 hospital, the treatment time will be from the time of admission in the 1st hospital (upto 48 hours only).
NK 48 Guideline – Preauth
Pre-auth submission by Hospital
Within 4 hours of admission during 8 am to 6 pm.
Within 12 hours of admission during 6 pm to 8 am
PREAUTH CRITERIA
Any Identification Card.
If there is no Identity Card, a letter from Hospital to be submitted.
Patient’s Clinical Photo.
Preliminary Assessment Report duly certified by examining Doctor.
AR copy with treating Doctor’s sign.
If the patient needs additional treatment or procedure, Enhancement request may be applied with Secondary Survey report.
CLAIMS CRITERIA
Treatment Summary, Discharge Summary / Referral Letter/ Death Summary within 5 days from the date of admission.
Declaration that no money has been collected from the patient during the course of treatment
CMCHIS URN if available.
All investigations done, with Images.
Operative notes and Case sheet.
Hospital Bills (detailed).
IKT – NK 48 Claims
Claims settlement for NK 48 within 3 days from Claim submission.
CMCHIS call center will make telephonic enquiry on the patient status and keep a record.
Any Death within 1 month of major accident should be reported with PM report for record maintenance.
NK 48 Guideline
Strict follow-up and bench marking of hospitals as per TAEI standards.
Frequent Audits for quality of care
List of Packages
S.NO
Package Name
Rate (in Rs.)
1
TA001 : Central line
4000
2
TA002 : Intraosseous line
4000
3
TA003 : Cervical Collar (philadelphia)
1500
4
TA004 : Endotracheal Intubation
2000
5
TA005 : Tracheostomy
10000
6
TA006 : Oropharngeal Airway
2000
7
TA007 : Blood and Blood Component Transfusion
2000
TA007a : Blood and Blood Component Transfusion – additional uit
Short thread on how kickass our TN Government health services is! I am super impressed and wanted to share this with everyone. @NHM_TN@Vijayabaskarofl 1/n
Short thread on how kickass our TN Government health services is! I am super impressed and wanted to share this with everyone. @NHM_TN @Vijayabaskarofl 1/n
At 9 pm approx (13 July), my security guard rings my doorbell sweating profusely, complaining of chest pain. We were in the midst of dinner and were totally unprepared for this. 2/n
Managed to get through to 108 in three tries and the ambulance reached us in less than ten minutes. The call centre girl was efficient and patched us to the ambulance driver quickly.
Both of them ask me mandatory Covid related questions and then a few more questions on exact location and asked us to have someone stand on the street, outside my building. 4/n
The Male nurse from the get-go, was extremely good. Handled the patient well… polite, respectful and empathetic. Once in the ambulance (in which I travelled along), he had a tough time with the patient who was unwilling to lie down, wouldn’t keep the oxygen mask on etc. 5/n
Kept his cool through out, while he tried to check his vitals and then put a line in, which was a struggle, as the man was totally uncooperative. Pretty soon, we were at Royapettah Hospital. 6/n
Now, this was perhaps my first time inside a proper government hospital…. I was impressed. The young doctors and nurses in the Triage section were great. The male nurse from the ambulance worked smoothly with them, like he was a member of staff. 7/n
All of them seemed to work hurriedly, as they handled about 15 patients and related attenders in the Emergency room. All with a great sense of purpose and no chaos at all. 8/n
Our patient needed to be pinned down, as he refused O2, pulled out the line which was inserted earlier etc. Big ups to all the nurses, who were super patient while taking his ECG, putting a new line & then calming him down (with some sedative I guess). 9/n
I step out of the emergency room to the car park to meet my driver who has now arrived. The male nurse from earlier has finished all his work and is walking back to the ambulance. 10/n
Now, the MAIN part… I holler and walk up to him… tell him I want to give him something… he says NO… I try again, this time actually bringing out a small wad of notes and he could see it was 500s… but again he said NO and said ’We are not supposed to take, brother!’ 11/n
There was nobody near us. This guy was real!! I couldn’t believe this. I’ve been in similar situations with the upmarket ambulance service (extremely professional), which came at a certain price & ending up in a private hospital, only to be hassled for tips by the lift boy! 12/n
I was so happy that this is the current scene in Chennai and I must say, I am loving it! Respect to these doctors and healthcare workers who are working selflessly, during these trying times. 13/n
Please do not speak disparagingly of TN Health services, if you have never experienced it. Love Chennai! Jai Hind!@Vijayabaskarofl @NHM_TN 14/n
Lastly, for those who asked, the patient is stable now. 15/15
( I) Teach the People that their expectation is unrealistic and can never be met and that if their unrealistic and impractical expectations are not met, it does not become negligence
I will explain this first
99.99 % of Our People who criticize Doctors want
1. All diseases cured in one day
2. by the treatment of their choice (if they want surgery, we have to operate : If they don’t want surgery, we have to resect meningioma with tablets) [Meningioma : A Tumour inside Skull]
3. Free of Cost
4. In the Hospital of their choice (Treatment of Myalgia in neurosurgery OP, Cardiac Bye Pass in Banavaram PHC) [Myalgia : Muscle Pain, usually due to work]
5. At the time they like (They will want admission of OA Knee at 11 PM) [OA Knee : Knee pain]
6. All diseases to be diagnosed at once
7. With the modality of their choice. If they want MRI Brain, we have to take it even when patient is fully conscious following fall from bicycle. If they don’t want, we shouldn’t get CT Brain done even if there is anisocoria
8. And doctors say what they like. You should always say that the disease does not need hospitalization if they are not ready for hospitalization. You should always not suggest surgery if they are not ready for surgery.
-oOo-
If any one of these conditions are not met , they will say that
1. Doctors are Negligent
2. Doctors are money minded
3. Doctors are not duty conscious
4. Doctors do not have accountability
5. Doctors did not tell me anything
6. Doctors did not explain treatment plan
eg :
If they want the diease to be cured in one day, but it takes 5 days, and even though the doctor has explained everything, they will still say that doctor did not explain me treatment plan / doctor did not tell me anything
eg
When they are told that Open Heart Surgery cannot be done at Banavaram PHC, they will say that Doctors are money minded (they do open heart surgery in their private clinic but not in PHC), Doctors are not duty conscious, Doctors do not have accountability
-oOo-
In this case, They wanted Neurosurgery in the hospital they first come
When it is not there
They consider that the doctor is negligent
and try to kill him
-oOo-
The issues are two fold
1. Lack of resources
2. Over expectation of people
The second is the main issue nowadays . . and when the people are at fault, they have to be blamed
-oOo-
99.99 % of Our Public distrust is because of their wrong, illogical, impractical expectation
The mistake has to be identified and solved
They need to be educated about reality
-oOo-
You please ask 1000 non medical people to list what they consider as 10 problems in health care
You will have a list of 10000 problems
9999 will come under the eight categories mentioned above
Tell straight on the face of the patients that what they expect is unrealistic and that they have to accept the reality
-oOo-
(II) Exclude Health Care from Consumer Courts
Health care is not consumerism
The Customer is King approach does not work here Health care is NOT Patient vs Doctor issue It is doctor + patient on one side and Disease on other side
Patients do have a lot of role to play in evolving a good health care system and if the system is in disarray they do have lot of blame to shoulder
Bringing health care under consumer courts is the single most anti people act in the history of health care
Wherever and whenever there is a blame from patient side, blame it is on patient side
Do not blame the doctor even when the patient is at fault
-oOo-
(III) A strict law absolving a doctor / group of doctors or healthcare professionals,, from any legal implications for any act of self defense while on duty
(IV) Increase Severity and Certainty of Punishment
Certainty of punishment is more important and helpful than severity of punishment in preventing a crime. This is what Australia Government has done
(V) Stop Defending the Criminal
Few Men rape
They do because of perversion and also because they consider the girl or woman as soft target.
They are emboldened because they know that there are people who will blame the girls dress as cause of rape
It is perversion to find reasons from the girls side in a rape
It is stupidity to suggest that there won’t be rapes if all women wear burqa
Rape can never be prevented by changing the dress of woman
The man is at fault
He needs to be changed.
-oOo-
Few people attack hospitals and health care professionals
They do because of perversion and also because they consider the hospital or health care worker as soft target.
They are emboldened because they know that there are people who will blame the hospital bill or overcrowding as cause of attack
It is perversion to find reasons from the hospital side in a rape
It is stupidity to suggest that there won’t be attacks on hospitals if all govt hospitals give Apollo services or if all private hospitals treat free
Hospital attacks can never be prevented by changing the hospital bill
The attacker is at fault
He needs to be changed.
-oOo-
Imagine two scenarios
Scenario 1 :
A pervert finds a girl child alone on the street and thinks of molesting her.
He has read in the news paper about a hundred similar incidents in past few weeks following which the criminal was given bail immediately and no conviction at all. In addition to the criminal being let free by the legal establishment, he has also seen fools / stupids / perverts wearing mask of intellectuals had discussed the various causes like Dress of the Victim, Victim coming alone, the emotion of the criminal etc as reasons and were talking against punishing the previous criminal and suggested that changes should start from victim’s dress and victims behaviour
He gets emboldened that even if he commits the crime,
1. he will come out in bail in one day,
2. he won’t be convicted
3. there will be enough fools / stupids / perverts wearing mask of intellectuals who will support him directly and indirectly
Scenario 2 :
A pervert finds a girl child alone on the street and thinks of molesting her.
He has read in the news paper about a similar incidents following which all the criminals were convicted and are in jail and every one was unanimous is giving 14 years imprisonment to the criminal
He will just back off if that news comes to his mind
-oOo-
Reason for increase in Sexual Violence against women
1. Perverts
2. Low Conviction Rate
3. Fools / stupids / perverts wearing mask of intellectuals who blame the Victim’s dress, victim’s behaviour and suggest that victim should change
Reason for increase in Hospital Attacks and Assaults on health care worker
1. Perverts in Public
2. Zero Conviction Rate
3. Fools / stupids / perverts wearing mask of intellectuals who blame the Hospital Bill or Hospital Waiting Time
-oOo-
Solution for Reducing Attack on Hospital
Legislature
1. Increasing Punishment to 14 years
2. Making Hospital Attacks as Non Bailable Offence
Executive
3. Time Bound Legal Procedure. 7 days for Filing Charge Sheet
Judiciary
4. Trial within 1 month
Civil Society aka Fools / stupids / perverts wearing mask of intellectuals
5. Stop Justifying the attacks
6. Stop Blaming the Victim
7. Stop Finding Imaginary Reasons
(VI) Include the details of these attackers in their Aadhar Card and form a PIBIL
Soon EMR (Electronic Medical Records) will be linked to Aadhar card. Just like CIBIL ( CREDIT INFORMATION BUREAU (INDIA) LIMITED), We need to have a PIBIL (Patient Information Bureau India Limited) linked with Aadhar Number and Entries made in the Aadhar Database of All the patients and attackers who cause trouble in hospital
So that
Other hospitals can use that to anticipate trouble and be prepared
First Attack : The Individual Should be banned from entering any health care facility all over India (Govt or Private) for a period of six months
Second Attack : The Individual Should be permanently banned from entering any health care facility, even for emergencies
Is this Ethical ?
Yes.
Hippocrates Oath becomes null and void for those who endanger the life of Other patients in the hospital as well as Health Care Providers
Key Points from the Narration & my Comments (in Bold Italics)
1
The police was very very helpful. They asked the crowd to keep away and got hold of the bolero driver.
There is a common misconception among people that Police do not help people or behave mechanically. The reality is always the other way round
2
I immediately gathered all my strength and asked for water & lime juice with salt. The police arranged immediately.
Police go to the extent of Helping the accident victim with the drink of his choice 🙂 🙂 That is really appreciable. But at the same time, we need to also educate the police and in case the patient requires surgery, it is better to keep the stomach free of any fluids. Of course, accident victims will feel thirst due to two mechanism (1) Blood Loss –> Hypovolemia (2) Sympathetic System Surge –> Dry Mouth , but don’t give anything by mouth till treatment plan is finalised
3
They also called the 108 and took me to Sankagiri GH.
4
Once inside the ambulance, I asked the attendar in the ambulance to remove my shoes and throw them away as they were out of shape and I could get some fresh air.
5
04:55 pm –
Sankagiri GH team received me with full speed, no time wasted they started first aid. Most painful moment of my life. Just a small pain killer given – no sedation – my big open wound was stitched and packed like a Rambo movie.
Please note that the GH Team had received immediately – 🙂 No Sedation Given – Because head injury is not yet ruled out. Any Sedation will lead to difficulty in accessing the neurological status if the patient’s consciousness goes down either due to head injury or due to blood loss6. Sankagiri GH has completed the First Aid + Wound Management in 20 minutes. In Singapore and UK, the average waiting time in ER is in hours while in TN we see that
Accident : 4:40 PM
Ambulance takes Patient to Hospital : 4:55 PM
Hospital completes First Aid & Wound Management : 5:15 PM
Very Few Countries can match this efficiency. And Remember. All these are done without patient paying a single paisa or even worrying about payment or having to fill forms etc
6
05:15 pm – Sankagiri GH process was over. We knew that golden moments should not be wasted. Mahesh bro came in his Thar jeep. The GH team made me sit comfortably on the back of the Jeep and we headed towards KMCH.
The GH team made me sit comfortably – Shows the Empathy
-oOo-
Full Narration Follows
What happened to me?
Lot of calls, messages enquiring about my health. Something went wrong and it is no fault that people who love me with lot of attention & care want to know what happened to me? – I can very well understand this curiosity is due to the care and affection.
I am bound to explain what happened to all of you. Due to my current position, I am explaining as short as possible about what happened.
Tue 15th Jan
07:00 am – Started on a ride to Pondy with the Lone Wolves
10:00 pm – Met with Pondy paleo friends at the beach
Wed 16th Jan
03:00 am – Had a great peaceful time with friends at the beach. Slept
07:00 am – Went to Vedhapureswarar temple, had a great darshan
11:00 am – Ride out from Pondy headed back home
03:00 pm – Had a good lunch at Ayodhipattinam before Salem
03:45 pm – Refuelled at Salem
04:15 pm – Felt sleepy, slept on the pavement of closed tea shop, was a good power nap
04:30 pm – Got up fresh, started riding back
04:40 pm – 4 kms after Sankagiri, was riding very slow, suddenly a bolero disappeared from nowhere without stopping to see from the other side service lane and came into enter this side service lane. I tried to avoid and ride to the left – could not avoid – got hit by the bolero on my right knee and was thrown yards away landing on the foot of a tea shop on the service lane. After the fall, I tried to get up. I sat up. There was police nearby. They rushed to my rescue. Somebody from the crowd tried to touch my helmet. I yelled at him to stay away and not to touch me. I consciously removed my ray ban, and then slowly my helmet making sure there was no dent in the helmet. The police was very very helpful. They asked the crowd to keep away and got hold of the bolero driver. I could see my right leg almost ripped on into two. How lucky a man is to see his own leg bones. 🙂 🙂 🙂
I immediately gathered all my strength and asked for water & lime juice with salt. The police arranged immediately. They also called the 108 and took me to Sankagiri GH. Once inside the ambulance, I decided not to make any unwanted calls fearing I would faint any time seeing the wound up close and blood that was flowing. I asked the attendar in the ambulance to remove my shoes and throw them away as they were out of shape and I could get some fresh air.
The first call I made was to my friend & brother Maheshwaran Nallaiyan from Tiruchencode as he was the nearest person I could reach from Sankagiri. I was very sure that even if he was not at home, he will arrange someone to take care of me immediately. My luck he was at home & his driver was at Sankagiri already for some work. He said his driver will reach GH first immediately & he will come there in 10 mins. That was a great relief to have a loved one nearby.
The second call I made was to my brother Dr. Dharani Subramaniam explained my situation and asked what to do. Dharani said do not panic. If you can remember me, call me without any chaos in such a situation you are mentally all well. He told me to finish GH first aid and head straight to KMCH, Coimbatore immediately without hesitation. Within 5 mins, Dharani called me back – said that all arrangements to receive me has been arranged by the top medics team at KMCH, Coimbatore at Emergency. He also said that he is on the way already to KMCH.
All this happened in a time of 10 minutes.
04:55 pm – Sankagiri GH team received me with full speed, no time wasted they started first aid. Most painful moment of my life. Just a small pain killer given – no sedation – my big open wound was stitched and packed like a Rambo movie.
Mahesh bro arrived at the GH when the first aid was going on and caught my hand offering strength.
05:15 pm – Sankagiri GH process was over. They called for a private ambulance who said he will come in one hour. We knew that golden moments should not be wasted. Mahesh bro came in his Thar jeep. The GH team made me sit comfortably on the back of the Jeep and we headed towards KMCH.
05:30 pm – I call and inform Mom that i met with a small accident – repeatedly said her not to panic and start immediately to KMCH. Mahesh bro drove me very comfortably keeping me occupied talking all the way so I should not sleep.
07:10 pm – I arrive at KMCH and get admitted at Emergency
07:20 pm – Dr. Dharani arrives check my wound and says not to worry we are in best hands.
07:30 pm – Doctors start checking my wound taking photos sending to seniors – deep discussion starts and Dr.Dharani is with them.
08:00 pm – More pain – they again wash my wound and make new dressing
08:10 pm – Taken to Xray
08:50 pm – Taken to CT scan – discussion continue with results
11:45 pm – Taken to Operation Theatre – Procedure 1 begins
It was a 2 hour long procedure thoroughly cleaning my wound so that no infection spreads in my body due to the external particles from the road
Thu 17th Jan
03:15 am – Reached room
10:00 am – Got up, rest day
Recoup the accident. I knew how i fly. Had there been an impact to my helmet, it should have been fatal. Lucky to be alive. It was my death day. Only Lord Shiva saved my life ending it with just a hit.
Fri 18th Jan
12:30 pm – Taken to Operation Theatre – Procedure 2 begins
It was the ortho procedure. Ortho surprised that my bone was damn strong to take such a beating. Just one minor fracture – fixation done with a bio collapsible tiatinium screw. No further damange – only scratches, will be healed by itself in a month – The effect of regular bone broth & vitamin d
06:00 pm – Reached room
Sat 18th Jan – Rest day
Sun 20th Jan – Doctor visits, remove dressing and fixes next procedure on Monday
Mon 21st Jan
02:00 pm – Taken to Operation Theatre – Procedure 3 begins
Again wound cleaning. Total dead skin removed.
06:00 pm – Reached room
Tue 22nd Jan
11:00 am – Dressing removed and VAC machine fixed to heal the wound faster
 Consciousness and Awareness have different meanings when used as Adjective
Consciousness and Awareness have different meanings when used as Adjective


 முதலுதவிக்கு 1 லட்சமா என்று கேள்வி எழுகிறதா ?
முதலுதவிக்கு 1 லட்சமா என்று கேள்வி எழுகிறதா ? முதல் வகை + இரண்டாம் வகை இரண்டுமே ஸ்பாட் அவுட் தான்
முதல் வகை + இரண்டாம் வகை இரண்டுமே ஸ்பாட் அவுட் தான் இதனால் என்ன பலன்?
இதனால் என்ன பலன்?

 Imagine two scenarios
Imagine two scenarios That is really appreciable. But at the same time, we need to also educate the police and in case the patient requires surgery, it is better to keep the stomach free of any fluids. Of course, accident victims will feel thirst due to two mechanism (1) Blood Loss –> Hypovolemia (2) Sympathetic System Surge –> Dry Mouth , but don’t give anything by mouth till treatment plan is finalised
That is really appreciable. But at the same time, we need to also educate the police and in case the patient requires surgery, it is better to keep the stomach free of any fluids. Of course, accident victims will feel thirst due to two mechanism (1) Blood Loss –> Hypovolemia (2) Sympathetic System Surge –> Dry Mouth , but don’t give anything by mouth till treatment plan is finalised