ஒருவருக்கு பைல்ஸ் பிரச்சனை அல்லது சிறுநீரக கோளாறு இருக்கிறது என்று வைத்துக்கொள்ளுங்கள்.
இப்பொழுது அவர் வைத்தியம் செய்து கொள்ள நிறைய இடங்கள் உள்ளன
- 1. அரசு மருத்துவமனையில் – இலவசமாக
- 2. தனியார் மருத்துவமனையில் – காசு கட்டி
- 3. தனியார் மருத்துவமனையில் – காப்பீடு மூலம் (அதாவது ஏற்கனவே காப்பீடு திட்டத்தில் சேர்ந்திருந்தால்)
எந்த மருத்துவமனை செல்வது என்பதை தீர்மானிக்க அவருக்கும் அவரது குடும்பத்தினருக்கும் நேரம் உள்ளது.
அவர் தனியார் மருத்துவமனையில் சேர்கிறார் என்றால், அவர் பணம் கட்டுவார் அல்லது அவரது காப்பீடு திட்டத்தை வைத்து அந்த மருத்துவமனை காப்பீடு நிறுவனத்திற்கு விண்ணப்பிப்பார்கள். அப்படி விண்ணப்பித்தவுடன், அந்த நிறுவனம் அதை அங்கீகரிக்கும். அதை வைத்து சிகிச்சை துவங்கும்
அவசரமில்லாத சிகிச்சைகளுக்கு இந்த பிரச்சனை இல்லை ஆனால் விபத்துக்களில் சிக்கல் உள்ளது
-oOo-![]()
அடி சிறிது என்றால் – சிராய்ப்பு மட்டும் தான் என்றால்- முதலுதவி சிறிது தான், சிகிச்சையும் சிறிது தான்.
ஆனால் அடி பலம் என்றால் – தலைக்காயம் அல்லது விலா எலும்பு முறிவு, கை கால் எலும்பு முறிவு என்றால்- முதலுதவியும் அதிகம், சிகிச்சையும் அதிகம்.
உதாரணமாக,
சிராய்ப்பு என்றால் முதலுதவிக்கு 100 ரூபாய் ஆகும். மொத்த வைத்தியம் ரூ500 முதல் ரூ1000 வரை ஆகும்.
கை எலும்பு முறிவு என்றால் முதலுதவிக்கு 1000 ரூபாய் ஆகும். மொத்த வைத்தியம் ரூ10000-ரூ30000 வரை ஆகலாம்.
கால் எலும்பு முறிவு என்றால் முதலுதவிக்கு 10000 ரூபாய் ஆகும். மொத்த வைத்தியம் ரூ1 லட்சம் – ரூ2 லட்சம் வரை ஆகலாம்.
தலைக்காயம் / முதுகு எலும்பு முறிவு என்றால் முதலுதவிக்கே ரூ1 லட்சம் ஆகும். மொத்த கட்டணம் ரூ3 லட்சம் முதல் ரூ10 லட்சம் ஆகலாம்
இது புரிந்து கொள்ளத்தான். சரியான கட்டணம் என்பது நபருக்கு நபர் மாறுபடும்.
-oOo-
 முதலுதவிக்கு 1 லட்சமா என்று கேள்வி எழுகிறதா ?
முதலுதவிக்கு 1 லட்சமா என்று கேள்வி எழுகிறதா ?
1980களில் முதலுதவி என்பது கட்டு போடுவது + வலிக்கு மாத்திரை அளிப்பது மட்டுமே. 1980களில் முதலுதவி என்பதை ஒரு சிறிய பெட்டிக்குள் அடக்கி விடலாம்
2021ல் முதலுதவி என்பதே பெரிதாகிவிட்டது
Philadelphia Collar / Spine Board / Pelvic Binders / Splints
Suction / OP Airway / NP Airway / Intubation / Tracheostomy
Ventilatory Suppor
Venflon / Central Line
Stat Lab
Volume Replacement Blood Transfusion
X Ray / eFast / CT / MRI
ICD / Pericardiocentesis
எனவே இன்றைய தேதிக்கு
உண்மையான முதலுதவி என்பது விபத்தின் தன்மையை பொருத்து 10 ரூபாயில் இருந்து (சிராய்ப்பு என்றால்) ரூ1 லட்சம் வரை (தலைக்காயம் + எலும்பு முறிவு + நுரையீரல் பாதிப்பு) ஆகும்.
-oOo-
சும்மா ஒரு கட்டு போட்டுவிட்டு, டிடி ஊசி போடுவது என்றால் 100 ரூபாய் செலவு. ஆனால் உண்மையில் உயிரை காக்க வேண்டும் என்றால் 1 லட்சம் செலவு.
சும்மா ஒரு கட்டு போட்டுவிட்டு, டிடி ஊசி போடுவது என்றால் 10 நிமிடம் தான் ஆகும். ஆனால் உண்மையில் உயிரை காக்க வேண்டும் என்றால் 6 மணி நேரம் வரை ஆகலாம்.
-oOo-
அந்த காலத்தில் எல்லாம் அடிபட்டால் 10 ரூபாய் தான் செலவு. இப்ப 1 லட்சமா, ஹாஸ்பிட்டல் எல்லாம் கொள்ளையடிக்கிறாங்க என்று புலம்புகிறீர்களா ?
சற்றுப் பொறுங்கள்.
விபத்தினால் நேரும் மரணங்களை கீழ்க்கண்டவாறு பகுக்கலாம்.
(1) முதல் வகை: மூளை, இதயம், மகாதமணி, முதுகுத்தண்டு ஆகியவை கிழிபடுவதால் ஏற்படும் உடனடி மரணம் – இது அடிபட்ட சில நொடிகளில் இருந்து 10 நிமிடங்களுக்குள் ஏற்படும். இதில் உயிரை காக்க வாய்ப்பு குறைவு. விபத்தை தடுப்பதன் மூலமே இதை தடுக்க முடியும்.
(2) இரண்டாம் வகை : மண்டக்குள் இரத்தக்கட்டு, நுரையீரலை சுற்றி இரத்தம் கட்டுவது, இதயத்தை சுற்றி இரத்தம் கட்டுவது, இரத்தப்போக்கு, மூச்சுத் திணறல் ஆகியவற்றால் ஏற்படும் மரணங்கள். இவை 10 நிமிடங்களில் இருந்து 2-3 நாட்களுக்குள் ஏற்படும். ஆனால் அடிபட்ட உடனே, அடிபட்ட 1 மணி நேரத்திற்குள் சிகிச்சையை அளிப்பதன் மூலம் இவர்களின் உயிரை காக்க முடியும்.
(3) மூன்றால் வகை : பிற அடிகள்.
-oOo-
1980களில் முதலுதவி என்பது கட்டு போடுவது + வலிக்கு மாத்திரை அளிப்பது மட்டுமே. 1980களில் முதலுதவி என்பதை ஒரு சிறிய பெட்டிக்குள் அடக்கி விடலாம். காரணம் அன்றைய காலக்கட்டத்தில் நாம் மூன்றாம் வகை அடிகளுக்கு மட்டும் தான் முதலுதவி செய்து வந்தோம்.
அன்றைய காலக்கட்டத்தில்
மண்டைக்குள் இரத்தக்கட்டு, நுரையீரலை சுற்றி இரத்தம் கட்டுவது, இதயத்தை சுற்றி இரத்தம் கட்டுவது, இரத்தப்போக்கு, மூச்சு திணறல் ஏற்பட்டால் மரணம் தான்.
அதாவது 1980களை பொருத்தவரை,
 முதல் வகை + இரண்டாம் வகை இரண்டுமே ஸ்பாட் அவுட் தான்
முதல் வகை + இரண்டாம் வகை இரண்டுமே ஸ்பாட் அவுட் தான்
ஆனால் 2021ல் நவீன அறிவியல் மருத்துவம் வளர்ந்த பிறகு இரண்டாம் வகைக்கு சிகிச்சை வந்துள்ளது. அதன் மூலம் உயிரை காக்க முடிகிறது. ஆனால் இதற்கு ரூ3 லட்சம் முதல் 10 லட்சம் வரை ஆகிறது. இந்த முதலுதவிக்கே ரூ1 லட்சம் ஆகிறது
அந்த காலத்தில் அடி பட்டு “ஸ்பாட் அவுட்” என்று கணக்கில் வந்தவர்களில் பாதி பேரை காக்க முதலுதவிக்கே 1 லட்சம் ஆகிறது.
அதாவது 10 ரூபாய் கட்டு போதுவது 1 லட்சம் ஆகவில்லை, புதிதாக 1 லட்சத்திற்கு சிகிச்சை வந்துள்ளது.
-oOo-
ஒருவர் சாலையில் செல்லும் போது விபத்துக்காகிறார் என்றால், அவர் கையில் 1 லட்சம் இருந்தால் அவருக்கு தனியார் மருத்துவமனையில் சிகிச்சை அளிப்பதில் எந்த பிரச்சனையும் இல்லை.
அவர் கையில் காசு இல்லை என்றால் அந்த தனியார் மருத்துவமனைக்கு யார் காசு கொடுப்பார்கள்?
அவர் கையில் காசு இல்லை, ஆனால் அவரிடம் காப்பீடு உள்ளது. அந்த காப்பீடு எண் கையில் இல்லை. அந்த தனியார் மருத்துவமனைக்கு யார் காசு கொடுப்பார்கள்?
இது தான் இன்று வரை இருந்த நடைமுறைச் சிக்கல்.
-oOo-
உதாரணமாக
ஒருவருக்கு விபத்தில் கை எலும்பு முறிந்துள்ளது, இது வரை 108 அம்புலன்ஸ்
அவரிடம் பணம் இருக்கிறதா?, காப்பீடு உள்ளதா?, உறவினர்களால் பணம் செலுத்த முடியுமா? என்ற எந்த கேள்வியும் கேட்காமல்
அவரை அரசு மருத்துவமனைக்குத்தான் அழைத்து செல்லும். அங்கு சென்று அவருக்கு முதலுதவி செய்யப்படும்.
பிறகு உறவினர்கள் எல்லாம் வந்த பிறகு
1. அவர்களிடம் காசு இல்லை என்றால் அவர்கள் அரசு மருத்துவமனையில் சிகிச்சை தொடரலாம்.
2. அவர்களிடம் காசு அல்லது காப்பீடு இருந்தால் வேறு தனியார் மருத்துவமனை செல்லலாம்.
-oOo-
உதாரணமாக,
ஒருவருக்கு விபத்தில் கை எலும்பு முறிந்துள்ளது
அவரிடம் பணம் உள்ளது.
அவர் தனியார் மருத்துவமனை தான் செல்வேன் என்று சொன்னால் அம்புலன்ஸ் அவரை அங்கு அழைத்து செல்வார்கள்.
-oOo-
உதாரணமாக,
ஒருவருக்கு விபத்தில் தலையில் அடிபட்டு மயக்கமாகியுள்ளார். அவர் யார் என்றே தெரியாது. இது வரை 108 அம்புலன்ஸ்
அவரை அரசு மருத்துவமனைக்குத்தான் அழைத்து செல்லும். அங்கு சென்று அவருக்கு முதலுதவி செய்யப்படும்.
பிறகு உறவினர்கள் எல்லாம் வந்த பிறகு
1. அவர்களிடம் காசு இல்லை என்றால் அவர்கள் அரசு மருத்துவமனையில் சிகிச்சை தொடரலாம்.
2. அவர்களிடம் காசு அல்லது காப்பீடு இருந்தால் வேறு தனியார் மருத்துவமனை செல்லலாம்.
-oOo-
இப்பொழுது தமிழக அரசு கொண்டு வந்துள்ள திட்டம் என்ன?
முழுசிகிச்சையில் முதலுதவி பகுதியை மட்டும் தனியாக பிரித்து அந்த முதலுதவிக்கு தமிழக அரசு பணம் கொடுக்கும் என்பது தான்.
இந்த திட்டத்தின் மூலம்
விபத்தில் அடிபட்டவரை அரசு மருத்துவமனைக்குத்தான் கொண்டு வரவேண்டும் என்ற அவசியம் இல்லை.
அருகில் உள்ள தனியார் மருத்துவமனைக்கும் கொண்டு செல்லலாம். முதலுதவிக்கு அரசு பணம் கொடுக்கும் என்பதால்
மருத்துவமனையும் பணம் பற்றி கவலைப்படாமல் சிகிச்சையை துவங்குவார்கள். அவருக்கு முதலுதவி சீக்கிரம் கிடைக்கும்.
பிறகு அவரது உறவினர்கள் வந்த பிறகு அவர்கள் ஆற அமர முடிவு செய்து (இரண்டு நாட்களுக்குள்)
1. காசு அல்லது காப்பீடு இல்லை என்றால் அரசு மருத்துவமனைக்கு வரலாம்
2. காசு அல்லது காப்பீடு உள்ளது என்றால் அதே மருத்துவமனையில் தொடரலாம்
3. காசு அல்லது காப்பீடு உள்ளது என்றால் வேறு தனியார் மருத்துவமனை செல்லலாம்
-oOo-
 இதனால் என்ன பலன்?
இதனால் என்ன பலன்?
1. அடிபட்டவருக்கு : உதவி சீக்கிரம் கிடைக்கும். எனவே உயிரை காக்க வாய்ப்பு அதிகம். கை கால் ஆகியவற்றில் அடி பட்டிருந்தால் அந்த உறுப்புகளை காக்கவும் வாய்ப்பு அதிகம்.
2. உறவினர்களுக்கு : ஒருவர் விபத்தில் அடிபட்டார் என்பது அதிர்ச்சி தரும் செய்தி. அந்த நிலையில் அதே மருத்துவமனையில் தொடர்வதா, வேறு எங்கும் செல்வதா, எவ்வளவு காசு ஆகும், கையில் காசு உள்ளதா, கடன் வாங்குவதா, நகையை அடமானம் வைப்பதா என்ற முடிவு எடுக்கவேண்டாம்.
3. தனியார் மருத்துவமனைக்கு: அந்த நபர் அதே மருத்துவமனையில் சிகிச்சையை தொடர்ந்தால், அவர்களுக்கு வருமானம்.
4. அரசிற்கு : மக்களின் உயிரை காக்க முடியும்.
-oOo-
சும்மா இருப்பவர்களை கூட தனியார் மருத்துவமனைகள் பெரிய அடி இருப்பதாக காண்பித்து அதிக கட்டணம் வாங்க முடியுமா ?
முடியாது.
(1) 108 அம்புலன்ஸ்சில் ஒருவர் ஏறும் போதே அவரது உடல்நிலை என்ன என்பது குறித்து அவர்கள் பதிந்துவிடுவார்கள். அதை வைத்தே அவரின் முதலுதவிக்கு எவ்வளவு பணம் தேவை என்பதை சொல்லிவிடலாம்.
(2) விபத்து நடந்த பிறகு காவல் துறையினர் முதல் தகவல் அறிக்கை பதிவார்கள். அதிலும் காயங்களின் தன்மை இருக்கும்.
எனவே இந்த இரண்டையும் வைத்து
இது 100 ரூபாய் முதலுதவியா, (சிராய்ப்பா) 1000 ரூபாய் முதலுதவியா, (கை எலும்பு முறிவா) 10000 ரூபாய் முதலுதவியா, (தொடை எலும்பு முறிவா) அல்லது 1 லட்சம் முதலுதவியா (தலைக்காயம், வயிறு கிழிந்துவிடுவது) என்பதை எளிதில் கண்டு கொள்ளலாம்.
-oOo-
“காவல்துறையும் மருத்துவமனையும் சேர்ந்து ஊழல் செய்வார்கள், எனவே இந்த திட்டத்தை எதிர்க்கிறேன்” என்று கூறுகிறீர்கள் என்றால் avada kedavra என்பதை தவிர சொல்ல எதுவும் இல்லை.
மேலும் அறிந்து கொள்ள இந்த காணொளியை பார்க்கலாம்
மருத்துவம் தொடர்பாக மூத்த எலும்பியல் மருத்துவர் லோகநாதன் சார் அவர்களின் பிற காணொளிகளை இங்கு காணலாம்

IKT – 48 மணி நேரம் நம்மைக்காக்கும் இன்னுயிர் காப்போம் திட்டம்
- Creating Emergency Care Fund (IKT Fund)
- 50 Cr Assurance Mode
- Fix ceiling of up to Rs. 1 lakh per individual
- Empanelment of Government and Private Hospitals – 609
- Integrate the 48 hour cashless scheme with the existing CMCHIS scheme after 48 hours
- Selection of 81 Appropriate Packages
IKT Empanelled 609 Hospitals
| Government Hospitals | Private Hospitals | ||
| Level 1 Hospitals | 20 | 30 | 50 |
| Level 2 Hospitals | 74 | 157 | 231 |
| Level 3 Hospitals | 121 | 207 | 328 |
| 215 | 394 | 609 |
The Scope of coverage
- If a patient needs admission and minor procedure (listed) which does not exceed 48 hours stay the same may be done at the hospital he/she is being admitted.
- If the patient is not stable or requires procedures that may need Hospitalisation beyond 48 hours one of the following conditions may apply.
- Stabilization of the patient and Discharge to any empanelled Hospital if the patient needs further treatment which is covered under Chief Minister’s Comprehensive Health Insurance Scheme and is eligible for Coverage.
- Stabilization of the patient and Discharge to Government Hospital if the patient needs further treatment but the treatment is not covered under Chief Minister’s Comprehensive Health Insurance Scheme or eligible for Coverage.
- Stabilization of the patient and continuation of treatment in same Hospital or any other hospital of his / her choosing if the patient is not willing for transfer to Government Hospital (or) has private Insurance (or) willing to continue treatment as a paid patient.
IKT – Categories of patients who will benefit under NK – 48
All accident victims on road within TN border including tourists from other states and foreigners
- Accident victims brought by Good Samaritans
- Accident victims brought by family
- Accident victims who come by themselves
- Unknown accident victim brought by police, or Good Samaritans
- Mass casualty accident victims
IKT – NK 48 Exclusion criteria
- Assault injuries
- Domestic injuries
- Fall from height
- Injuries due to fall of heavy object
- Train traffic accident injuries
- Animal bites, Self harm
- Occupational work place injuries
- Thermal /Chemical/ Burn Injuries
- Cracker Blast Injuries
5 Steps of Emergency Trauma Care
- Prehospital Triage & Transportation by Ambulance along with in-transit care
- Resuscitation & Stabilization in hospital Emergency Department
- Damage Control Surgeries
- Definitive Care
- Rehabilitation
Step 1,2,3 – IKT
Steps 4,5 – KKT – CMCHIS
NK 48 Guideline
- On receipt of information from the accident site, Life support ambulance with trained manpower will reach the spot, Triaging & basic resuscitation (cABC) will be done by EMT.
- Patients maybe entitled for free treatment upto 48 hours in hospitals of IK – NK 48 Scheme empanelled private hospitals of neighbouring states if the accident occurs within Tamil Nadu but close to the state border.
NK 48 Guideline
5 Levels of triaging at the Accident Scene for guiding the EMT
| Pre-hospital Triage & Acuity Scale | Description of the Acuity Scale | Equivalent Triage category |
| Level 1 – Resuscitation | Patient battling for life in need of resuscitation/Severe hemodynamic compromise/Shock/Traumatic amputation of an extremity | Red |
| Level 2 – Emergent | Seriously injured patient who requires rapid medical intervention/Penetrating head,chest or abdominal injury/Neurovascular compromise of an extremity | Red |
| Level 3 – Urgent | Patient with stable vitals, but the presenting problem suggests further evaluation | Yellow |
| Level 4 – Less Urgent | Stable patient with lesser pain scale./ Laceration/Puncture requiring sutures/Isolated upper extremity injury | Green |
| Level 5 – Non-Urgent | Minor contusions, abrasions, lacerations not requiring closure, Non urgent with minor complaint | Green |
RTA – Patient comes to any Hospital
- IK NK 48 Basic Trauma Package for any RTA Patient – Clinical examination ,Hb, Urea, Sugar,ECG,X –Ray Chest. Patient is stable. He will be discharge (Green Category)
- Patient in Red / Yellow category
- CMCHIS Card Holder(Upto 48 hours) IK – NK48 Empaneled Hospital
- Treatment under IK – NK 48 Packages
- CMCHIS Non Card Holder / other state / Foreign RTA victims (Upto 48 hours) IK – NK48 Empaneled Hospital
- Treatment under IK – NK48 Packages
- CMCHIS Card Holder(Upto 48 hours) IK – NK48 Empaneled Hospital
- Packages applicable only Upto 48 Hours in the NK 48 empanelled 609 hospitals only. IFT Can be done within 48 hours based on the triage only among the NK 48 empanelled 609 hospitals
- After 48 Hours (Red & Yellow Category)
- CMCHIS Card holder Hospital ( Govt / Pvt empanelled Hospitals under CMCHIS)
- Treatment will be continued under CMCHIS as per existing packages
- Non CMCHIS Card holder ( Govt / Pvt empanelled Hospitals under CMCHIS)
- Treatment will be continued under free category in Govt Hospitals
- Treatment will be continued under payment / pvt insurance by the patient in pvt hospitals
- CMCHIS Card holder Hospital ( Govt / Pvt empanelled Hospitals under CMCHIS)
- Other state / foreign RTA victims
- Treatment will be continued under free category in Govt Hospitals
- Treatment will be continued under payment / pvt insurance / PM-JAY by the patient in pvt hospitals
NK 48 Guideline
- Critically ill (Red category) patient to be taken by 108 Ambulance service to the nearest empanelled Level 1 Hospital if located within 20-30km.
- The Level 1 Hospital may be a Government Hospital or a private facility.
- The patient should be transported in the shortest period to ensure advanced trauma life support.
- If it is far, the patient should be stabilized in the nearest L2 or L3 hospital and through 108 ambulance should move the patient after stabilization to the L1 facility for definitive intervention.
- 2 hr mandatory resuscitation for a critically injured patient before any Inter-facility Transfer.
- IFT with Pre-Arrival Intimation to the receiving hospital.
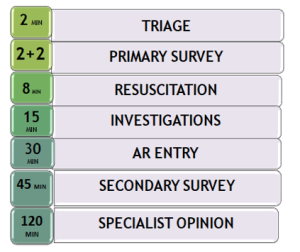
Time Norms in Emergency Care of RTA patients
NK 48 Guideline – Preauth & Claim
- EI number should be obtained by the treating hospital, & the URN should be shared even with IFT(Inter facility transfer) Hospital till the treatment course is completed under IKT.
- When treatment involves more than 1 hospital, the treatment time will be from the time of admission in the 1st hospital (upto 48 hours only).
NK 48 Guideline – Preauth
- Pre-auth submission by Hospital
- Within 4 hours of admission during 8 am to 6 pm.
- Within 12 hours of admission during 6 pm to 8 am
PREAUTH CRITERIA
- Any Identification Card.
- If there is no Identity Card, a letter from Hospital to be submitted.
- Patient’s Clinical Photo.
- Preliminary Assessment Report duly certified by examining Doctor.
- AR copy with treating Doctor’s sign.
- If the patient needs additional treatment or procedure, Enhancement request may be applied with Secondary Survey report.
CLAIMS CRITERIA
- Treatment Summary, Discharge Summary / Referral Letter/ Death Summary within 5 days from the date of admission.
- Declaration that no money has been collected from the patient during the course of treatment
- CMCHIS URN if available.
- All investigations done, with Images.
- Operative notes and Case sheet.
- Hospital Bills (detailed).
IKT – NK 48 Claims
- Claims settlement for NK 48 within 3 days from Claim submission.
- CMCHIS call center will make telephonic enquiry on the patient status and keep a record.
- Any Death within 1 month of major accident should be reported with PM report for record maintenance.
NK 48 Guideline
- Strict follow-up and bench marking of hospitals as per TAEI standards.
- Frequent Audits for quality of care
List of Packages
| S.NO | Package Name | Rate (in Rs.) |
| 1 | TA001 : Central line | 4000 |
| 2 | TA002 : Intraosseous line | 4000 |
| 3 | TA003 : Cervical Collar (philadelphia) | 1500 |
| 4 | TA004 : Endotracheal Intubation | 2000 |
| 5 | TA005 : Tracheostomy | 10000 |
| 6 | TA006 : Oropharngeal Airway | 2000 |
| 7 | TA007 : Blood and Blood Component Transfusion | 2000 |
| TA007a : Blood and Blood Component Transfusion – additional uit | 1000 | |
| 8 | TA008 : Chest tube / ICD | 4500 |
| 9 | TA009 : Nasogastric tube | 700 |
| 10 | TA010 : Urinary Catheter | 1000 |
| 11 | TA011 : X-ray – Per Region | 500 |
| 12 | TA012 : USG Fast / Pocus | 1500 |
| 13 | TA013 : Doppler | 2000 |
| 14 | TA014 : CT Plain | 1500 |
| TA014A : CT Contrast | 2000 | |
| 15 | TA015 : MRI Plain | 2500 |
| TA015A : MRI Contrast | 4000 | |
| 16 | TA016 : Blood typing & cross match | 500 |
| 17 | TA017 : Blood glucose | 50 |
| 18 | TA018 : CBC | 350 |
| 19 | TA019 : BT, CT, PT-INR | 400 |
| 20 | TA020 : APTT | 300 |
| 21 | TA021 : D-Dimer, Fibrin, FDP | 2450 |
| 22 | TA022 : Se. Amylase | 400 |
| 23 | TA023 : CK, CKMB (cardiac enzymes) | 1000 |
| 24 | TA024 : Blood Urea | 150 |
| 25 | TA025 : Se. Creatinine | 150 |
| 26 | TA026 : Electrolytes, | 400 |
| 27 | TA027 : Rhesus Antibody | 750 |
| 28 | TA028 : LFT | 450 |
| 29 | TA029 : Urine (Routine) | 150 |
| 30 | TA030 : ABG | 1500 |
| 31 | TA031 : HBs CMIA | 600 |
| TA031A : HBs Spot (Ag) | 300 | |
| 32 | TA032 : Anti HCV CMIA | 750 |
| TA032A : Anti HCV Spot | 350 | |
| 33 | TA033 : HIV 1& 2 Spot | 350 |
| TA033A : HIV 1& 2 p24 Ag/Ab | 500 | |
| 34 | TA034 : CT Angiogram | 6000 |
| 35 | TA035 : ECG | 200 |
| 36 | TA036 : Echocardiogram | 1500 |
| 37 | TA037 : Bronchoscopy | 3000 |
| 38 | TA038 : Cystogram (bladder) | 1500 |
| 39 | TA039 : Nasal Packing | 750 |
| 40 | TA040 : Surgical cricothyroidotomy | 2500 |
| 41 | TA041 : Needle cricothyroidotomy | 1500 |
| 42 | TA042 : Suprapubic catheterisation (surgical Procedure) | 3000 |
| 43 | TA043 : Pleural Aspiration | 2000 |
| 44 | TA044 : Nerve Block | 2000 |
| 45 | TA045 : Cardiac Tamponade – Aspiration | 2500 |
| 46 | TA046 : Wound exploration and Primary closure | 4000 |
| 47 | TA047 : Diagnostic Peritoneal Lavage | 5000 |
| 48 | TA048 : Peritoneal cavity – Tapping | 2000 |
| 49 | TA049 : Abdominal injuries necessitating obstetric evaluation | 4000 |
| 50 | TA050 : Bladder injuries – repair | 40000 |
| 51 | TA051 : Pelvic Fractures -Conservative – Binder | 3500 |
| 52 | TA052 : TMJ reduction | 3500 |
| 53 | TA053 : Facio Maxillary / Pan Facial injuries – (Non-surgical management) | 4000 |
| 54 | TA054 : Thoraco lumbar spine injuries – Conservative – Brace / Corset | 4000 |
| 55 | TA055 : Burns – (25 to 50%) collagen application) | 50000 |
| 56 | TA056 : Fasciotomy | 20000 |
| 57 | TA057 : Crush Injury of extremities Surgical management | 25000 |
| 58 | TA058 : Acute Renal Failure with HD / PD | 15000 |
| 59 | TA059 : Orbital trauma / intraocular FB with B-Scan | 5000 |
| 60 | TA060 : Lid Tears | 4000 |
| 61 | TA061 : Nerve / tendon/ soft tissue repairs | 25000 |
| 62 | TA062 : Limb salvage surgery / Amputation | 20000 |
| 63 | TA063 : Exploration under Anaesthesia for FB | 15000 |
| 64 | TA064 : Chest injuries – Damage control Surgery | 50000 |
| 65 | TA065 : Abdominal & Pelvic injuries – Damage control Surgery | 50000 |
| 66 | TA066 : Vascular injuries – Surgery | 60000 |
| 67 | TA067 : Emergency procedures for Increased ICP – Burrhole / Craniectomy | 45000 |
| TA067A : Emergency procedures for Increased ICP – Craniectomy | 70000 | |
| 68 | TA068 : Casts / POP | 4000 |
| 69 | TA069 : Splints | 9000 |
| 70 | TA070 : Closed reduction with casts / splints | 8000 |
| 71 | TA071 : Avulsion injury of Scalp – Surgical Management | 25000 |
| 72 | TA072 : Wound Dressings | 3000 |
| 73 | TA073 : Degloving Injury | 20000 |
| 74 | TA074 : Complete Primary Survey Yellow cases | 15000 |
| 75 | TA075 : Complete Primary Survey Red cases | 30000 |
| 76 | TA076 : Ventilator Charges | 200/hr |
| 77 | TA077 : NIV Charges | 100/hr |
| 78 | TA078 : DC Cardioversion – per shock | 1500 |
| 79 | TA079 : Fixed Daily charges – Ward | 2000 |
| 80 | TA080 : Fixed Daily charges – ICU | 4000 |
| 81 | TA081 : Broad-spectrum antibiotics and other highend drugs | as per drug bill / TNMSC Cost |
NK – 48 District Wise Empanelled Hospitals
| S.No | District | Govt | Govt total | Pvt | Pvt total | Grand total | |||||
| Level 1 | Level 2 | Level 3 | |||||||||
| Level 1 | Level 2 | Level 3 | |||||||||
| 1 | Ariyalur | 0 | 1 | 1 | 2 | 0 | 0 | 3 | 3 | 5 | |
| 2 | Chengalpattu | 1 | 3 | 0 | 4 | 9 | 5 | 0 | 14 | 18 | |
| 3 | Chennai | 8 | 0 | 0 | 8 | 2 | 8 | 0 | 10 | 18 | |
| 4 | Coimbatore | 2 | 1 | 14 | 17 | 3 | 7 | 43 | 53 | 70 | |
| 5 | Cuddalore | 0 | 1 | 5 | 6 | 1 | 1 | 1 | 3 | 9 | |
| 6 | Dharmapuri | 1 | 0 | 2 | 3 | 0 | 0 | 3 | 3 | 6 | |
| 7 | Dindigul | 0 | 7 | 1 | 8 | 0 | 25 | 0 | 25 | 33 | |
| 8 | Erode | 0 | 2 | 5 | 7 | 0 | 5 | 26 | 31 | 38 | |
| 9 | Kallakurichi | 0 | 1 | 4 | 5 | 0 | 1 | 12 | 13 | 18 | |
| 10 | Kancheepuram | 0 | 2 | 3 | 5 | 1 | 9 | 0 | 10 | 15 | |
| 11 | Kanyakumari | 0 | 0 | 2 | 2 | 0 | 2 | 9 | 11 | 13 | |
| 12 | Karur | 0 | 4 | 0 | 4 | 0 | 3 | 0 | 3 | 7 | |
| 13 | Krishnagiri | 1 | 1 | 5 | 7 | 0 | 0 | 14 | 14 | 21 | |
| 14 | Madurai | 1 | 0 | 5 | 6 | 3 | 5 | 5 | 13 | 19 | |
| 15 | Mayiladuthurai | 0 | 1 | 5 | 6 | 0 | 0 | 3 | 3 | 9 | |
| 16 | Nagapattinam | 0 | 1 | 4 | 5 | 0 | 0 | 1 | 1 | 6 | |
| 17 | Namakkal | 0 | 7 | 0 | 7 | 0 | 11 | 0 | 11 | 18 | |
| 18 | Nilgiris | 0 | 1 | 3 | 4 | 0 | 0 | 2 | 2 | 6 | |
| 19 | Perambalur | 0 | 1 | 0 | 1 | 1 | 0 | 6 | 7 | 8 | |
| 20 | Pudukottai | 0 | 1 | 2 | 3 | 0 | 2 | 2 | 4 | 7 | |
| 21 | Ramanathapuram | 0 | 1 | 3 | 4 | 0 | 0 | 3 | 3 | 7 | |
| 22 | Ranipet | 0 | 0 | 4 | 4 | 0 | 1 | 2 | 3 | 7 | |
| 23 | Salem | 1 | 1 | 6 | 8 | 1 | 10 | 12 | 23 | 31 | |
| 24 | Sivagangai | 0 | 7 | 0 | 7 | 0 | 11 | 1 | 12 | 19 | |
| 25 | Tenkasi | 0 | 0 | 3 | 3 | 0 | 0 | 1 | 1 | 4 | |
| 26 | Thanjavur | 1 | 0 | 5 | 6 | 2 | 2 | 12 | 16 | 22 | |
| 27 | Theni | 0 | 6 | 0 | 6 | 0 | 6 | 0 | 6 | 12 | |
| 28 | Thirupathur | 0 | 0 | 4 | 4 | 0 | 0 | 2 | 2 | 6 | |
| 29 | Tirunelveli | 1 | 0 | 0 | 1 | 0 | 2 | 8 | 10 | 11 | |
| 30 | Tiruppur | 0 | 1 | 7 | 8 | 1 | 4 | 16 | 21 | 29 | |
| 31 | Tiruvallur | 0 | 6 | 3 | 9 | 1 | 10 | 0 | 11 | 20 | |
| 32 | Tiruvannamalai | 0 | 1 | 5 | 6 | 1 | 0 | 0 | 1 | 7 | |
| 33 | Tiruvarur | 0 | 2 | 7 | 9 | 0 | 2 | 3 | 5 | 14 | |
| 34 | Trichy | 1 | 6 | 2 | 9 | 3 | 19 | 0 | 22 | 31 | |
| 35 | Tuticorin | 0 | 1 | 3 | 4 | 0 | 0 | 4 | 4 | 8 | |
| 36 | Vellore | 1 | 0 | 3 | 4 | 1 | 1 | 7 | 9 | 13 | |
| 37 | Villupuram | 1 | 0 | 5 | 6 | 0 | 1 | 5 | 6 | 12 | |
| 38 | Virudhunagar | 0 | 7 | 0 | 7 | 0 | 4 | 1 | 5 | 12 | |
| Total | 20 | 74 | 121 | 215 | 30 | 157 | 207 | 394 | 609 | ||
| Government Hospitals | Private Hospitals | ||
| Level 1 Hospitals | 20 | 30 | 50 |
| Level 2 Hospitals | 74 | 157 | 231 |
| Level 3 Hospitals | 121 | 207 | 328 |
| 215 | 394 | 609 |
Last, but not the least
Accident and life loss are unfair.
Let’s ensure we are FAIR.
- சீரான சாலைகள் அமைத்து
- நம்மை காக்கும் 48 சேவையில்
- அவசர மருத்துவ சேவைகள் சட்டம் பாதுகாக்க
- உயிரிழப்புகளை தவிர்த்து விபத்தில்லா தமிழ்நாடு உருவாக உதவி செய்து
- இன்னுயிர் காப்போம்