1
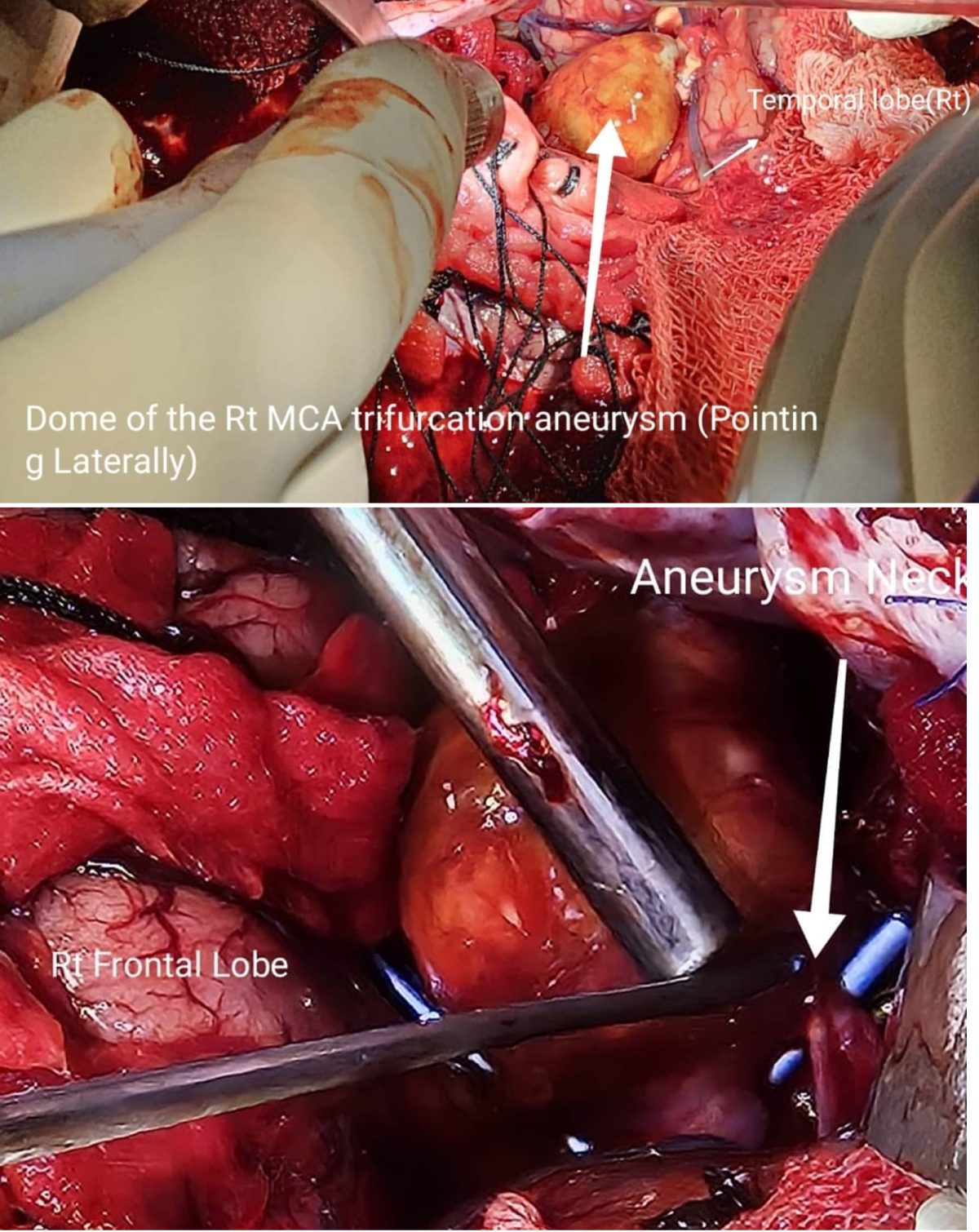
இரத்தக்குழாய்களில், தமனிகளில் ஏற்படும் வீக்கத்திற்கு தமனிக்கொப்புளம் என்று பெயர். இதை ஆங்கிலத்தில் அனிருசம் aneurysms என்று அழைப்பார்கள். மூளைக்குள் இருக்கும் தமனிகளில் சில நேரங்களில் இது போன்ற வீக்கங்கள் ஏற்படுவதுண்டு. இதை விட்டு விட்டால் எந்நேரம் வேண்டுமானாலும் இது வெடித்து அதனால் மூளைக்கும் இரத்தக்கசிவு ஏற்படலாம். சிறிதளவு மட்டுமே இரத்தம் கசிந்தால் சிகிச்சை அளித்து அந்த நபரை காப்பாற்ற முடியும். அதிக அளவு இரத்தம் கசிந்தால் அது உயிருக்கு ஆபத்தாக முடியும்
எனவே இது போன்ற வீக்கம் இருப்ப்தை கண்டு பிடித்தவுடன் அறுவை சிகிச்சை செய்து கிளிப் ஒன்றை அங்கு பொறுத்தி வீக்கம் வெடிக்காமல் செய்யவேண்டும். சில நேரங்களில் மூளையின் உள்ளே, எளிதில் அறுவை சிகிச்சை செய்ய முடியாத இடங்களில் வீக்கங்கள் இருந்தால் குருதி குழாய் வழியாகவே சுருள்கள் (coil) மற்றும் குருதி வழி திருப்பி (flow diverter) ஆகியவை மூலம் சிகிச்சை அளிக்கலாம்.
இவை அனைத்தும் மிகவும் நுணுக்கமான, நவீன கருவிகள் மற்றும் மிகுந்த திறன் தேவைப்படும் சிகிச்சை முறைகள்
பொதுவாகவே மூளையில் செய்யப்படும் அறுவை சிகிச்சை தேவைப்படும் படிப்பு, பயிற்சி, திறமை ஆகியவை அடிகம். அதனால் தான் அறுவை சிகிச்சை செய்யப்படும் பல மருத்துமனைகளில் மூளை அறுவை சிகிச்சை செய்யப்படுவதில்லை
இது போன்ற அறுவை சிகிச்சைகளை செய்ய 1. அறுவை அரங்கில் நுண்ணோக்கி (Operating Microscope) 2. நுண் அறுவை சிகிச்சை செய்யும் கருவிகள் (Micro surgery instruments) 3. மூளை அறுவை சிகிச்சை நிபுணர் (Neurosurgeon) 4. மயக்கவியல் நிபுணர் (Anaesthesiologist) 5. அறுவை அரங்க செவிலியர் (Theatre Nurse) 6. அறுவை அரங்க நுட்பனர் (OT Technician)
தேவை என்பதால் மூளை அறுவை சிகிச்சை செய்யப்படும் பல மருத்துவமனைகளில் கூட தமனிக்கொப்புளத்திற்கான அறுவை சிகிச்சைகள் செய்யப்படுவதில்லை.
பல நாடுகளில் இந்த அறுவை சிகிச்சை செய்யப்படுவதில்லை. இந்தியாவிலும் கூட சில மாநிலங்களில் செய்யப்படாததால் தான் நோயாளிகள் சென்னை வருகிறார்கள்
2
விழுப்புரம் அரசு மருத்துவக்கல்லூரி 2010ஆம் ஆண்டில் ஆரம்பிக்கப்பட்டது. தமிழகத்தில் இருக்கும் பல மருத்துவக்கல்லூரிகளை விட அது புதிது தான்.
3
மூளையில் உள்ள பெருமூளை நடுத்தமனியில் (MCA Middle Cerebral Artery) ஏற்பட்ட சிக்கலான முக்கூறு (Trifurcation) தமனிக்கொப்புளத்தால் (Aneurysm) பாதிக்கப்பட்ட நோயாளி ஒருவருக்கு விழுப்புரம் அரசு மருத்துவமனையிலேயே அறுவை சிகிச்சை செய்யப்பட்டுள்ளது. மூளை முதுகுத்தண்டு நரம்பியல் அறுவை சிகிச்சை நிபுணர்கள் மரு.பல்லவன், மரு.சந்தோஷ், மரு. ராஜ்கவுதம் ஆகியோருக்கு பாராட்டுக்கள்
தமிழக அரசு மருத்துவத்துறையில் இருக்கும் நவீன கருவிகள், மற்றும் மருத்துவர்களில் திறமை, அர்ப்பணிப்பு ஆகியவற்றில் ஆழத்தையும் அகலத்தையும் இது பறைசாற்றுகிறது
-oOo-
இதே போல் மூளையின் உட்கழுத்துத் தமனியில் (Internal Carotid Artery) ஏற்பட்ட தமனிகொப்புளத்திற்கு (aneurysm) சில நாட்கள் முன்னர் பிரபல தமிழ் திரைப்பட நடிகர் சென்னையின் தனியார் மருத்துவமனையில் சிகிச்சை பெற்றார். அதே பிரச்சனைக்கு, தனது வீட்டின் அருகிலேயே, முற்றிலும் இலவசமாக ஒருவருக்கு அறுவை சிகிச்சை செய்யப்பட்டுள்ளது.
189 வயதான மெட்ராஸ் மருத்துவக்கல்லூரியிலோ, அல்லது மதுரை, கோவை போல் தமிழகத்தின் ஓரிரண்டு இடங்களில் மட்டும் இது நடக்கவில்லை
தமிழகத்தில் 25க்கு மேற்பட்ட இடங்களில் இது போன்ற நவீன உயர்தர அறுவை சிகிச்சைகள் தினந்தோறும் நடந்து கொண்டு தான் உள்ளன
பல நாடுகளில் இந்த அறுவை சிகிச்சையை செய்யும் வசதி இல்லை
சில நாடுகளில் ஓரிரண்டு நிலையங்களில் மட்டுமே இதை செய்ய முடியும்
அதுவும் அமெரிக்கவில் இதற்கு கட்டணம் $138,000
தனது வீட்டில் இருந்து 50 கிலோமீட்டருக்குள் இருக்கும் ஒரு மருத்துவமனையின் மூளையில் ஏற்பட்ட தமனிக்கொப்புளத்திற்கு அறுவை சிகிச்சை செய்து கொள்ளவும் வசதி உள்ளதும் அதுவும் இலவசமாக செய்து கொள்ளலாம் என்பதும் தான் தமிழக மருத்துவத்துறையின் சிறப்பு
சில நாடுகளில் இந்த அறுவை சிகிச்சைக்கும் காலம் மிகவும் அதிகம் எனப்தால் தமனிக்கொப்புளம் வெடித்து விடுகிறது
-oOo-
மூளையில் இருக்கும் இரத்தக்குழாய்களில் வெடிப்பு ஏற்பட்டால் என்ன ஆகும் ?
வெடிப்பு ஏற்பட்ட இரத்தக்குழாய் என்ன வகையானது, அது எங்குள்ளது என்பதை பொறுத்து பல பிரச்சனைகள் வரலாம்
மூளைக்குள் இருக்கும் இரத்த குழாய்களில் வெடிப்பு ஏற்பட்டால் மூளைக்கு இரத்த கசிவு ஏற்படலாம் (Intra cerebral Hemorrhage)
அதே நேரம் மூளைக்கு செல்லும் தமணிகளில் வெடிப்பு ஏற்பட்டால் இரத்த கசிவு மூளையின் மேல் உள்ள மெல்லிய உரை (arachnoid membrane) மற்றும் மூளைக்கு இடையில் (sub arachnoid bleed) ஏற்படலாம்
இது போல் மூளைக்கும், மூளைக்கு வெளியில் இருக்கும் மெல்லிய உரையான அராக்னாய்ட் சவ்விற்கும் இடையில் ஏற்படும் இரத்த கசிவை Sub Arachnoid Hemorrhage என்று அழைக்கிறார்கள்
அப்படி ஏற்படும் போது
1. அந்த இரத்த கசிவு தொடர்ந்து கொண்டிருந்தால் நபர் இறந்து விடுவார்
2. (தானாக உறைந்து) இரத்த கசிவு நின்றால் கூட இரு வித பாதிப்புகள் ஏற்படலாம்
முதலாவதாக
இந்த மூளைக்கு வெளியில் இருக்கும் மெல்லிய உரையான அராக்னாய்ட் சவ்விற்கும் இடையில் உள்ள இடத்தில் (sub arachnoid space) மூளை தண்டுவட நீர் (CSF, Cerebro Spinal Fluid) இருக்கும். அதன் வழியாகத்தான் பிற இரத்தக்குழாய்கள் செல்லும். இந்த இடத்தில் இரத்தம் வந்தது என்றால் பிற இரத்தக்குழாய்கள் சுருங்கி (vasospasm) அதனால் மூளைக்கு செல்லும் இரத்த ஓட்டம் பாதிக்கப்பட்டு மூளையின் திசுக்கள் வேலை செய்யாமல் (ischemia) போகலாம். அல்லது இறந்து (infarct) போகலாம்
3
இரண்டாவதாக மூளை தண்டுவட நீரில் (CSF, Cerebro Spinal Fluid) இரத்தம் கலப்பதால் அந்த நீர் செல்லும் பாதையில் அடைப்பு ஏற்பட்டு, அந்த நீர் வெளியில் செல்லாமல், மூளைக்குள் அதிக அழுத்தம் ஏற்படலாம்
எனவே
ஒருவருக்கு மூளையின் மேல் உள்ள மெல்லிய உரை (arachnoid membrane) மற்றும் மூளைக்கு இடையில் இரத்தக்கசிவு ஏற்பட்டால் (sub arachnoid bleed) நாம் செய்யவேண்டிய விஷயங்கள் மூன்று
1.
எதனால் இரத்தக்கசிவு ஏற்பட்டுள்ளது என்பதை கண்டறிந்து அதை நிறுத்த முயலவேண்டும். மீண்டும் இரத்த கசிவு ஏற்படாமல் தடுக்க வேண்டும்
2.
இரத்தக்குழாய்கள் சுருங்கியிருந்தால் அதை விரிய வைக்க வேண்டும்
3.
மூளைக்குள் நீர் செல்லும் பாதையில் அடைப்பு ஏற்பட்டிருந்தால் நீர் வெளியேற மாற்றுப்பாதை கண்டு பிடிக்க வேண்டும்
-oOo-
1
எதனால் இரத்தக்கசிவு ஏற்பட்டுள்ளது என்பதை கண்டறிய உள்ளுறுப்பு ஊடு பதிவி இரத்தநாளச் நிழல் படம் (சிடி ஆஞ்சியோ) அல்லது எண்ணிம இரத்தநாள நிழல் படம் (digital subtraction angiogram) செய்ய வேண்டும்
2
இரத்தக்குழாய்கள் சுருங்கியிருந்தால் அதை விரிய வைக்க மருந்து கொடுக்கவேண்டும்
3
மூளைக்குள் நீர் செல்லும் பாதையில் அடைப்பு ஏற்பட்டிருந்தால் நீர் வெளியேற அறுவை சிகிச்சை மூலம் மாற்றுப்பாதை ஏற்படுத்த வேண்டும்
4.
எதனால் இரத்தக்கசிவு ஏற்பட்டுள்ளது என்பதை கண்டறிந்த பிறகு அந்த பிரச்சனைக்கு அறுவை சிகிச்சை மூலமோ ஆஞ்சியோ மூலமோ வைத்தியம் செய்யவேண்டும்
-oOo –
மூளைக்குள் இரத்தக்குழாய் வெடிக்கும் போது அது பெரிய வெடிப்பு என்றால் அந்த நபர் இறந்து விடுவார்
சிறு வெடிப்பு என்றால் தலைவலி வரும்
-oOo –
நடைமுறையில் என்ன நடக்கிறது என்றால்
தலைவலியுடன் மருத்துவமனை செல்பவருக்கு ஸ்கேன் செய்து பார்த்து விட்டு இரத்த கசிவு என்று சொல்வார்கள்
எங்கு என்று சொல்லமாட்டார்கள். ஏனென்றால் அவர்களுக்கே தெரியாது
அடுத்து இரத்தக்குழாய்கள் சுருங்கியிருந்தால் அதை விரிய வைக்க மருந்து கொடுக்கவேண்டும் என்பதால் தீவிர பிரிவில் வைத்திருப்பார்கள்.
ஒரு வேளை அழுத்தம் அதிகரித்தால் அதற்கு அறுவை சிகிச்சை செய்யவேண்டும் என்பார்கள். இந்த அறுவை சிகிச்சையினால் இரத்த கசிவு நிற்காது என்று மருத்துவர்கள் கூறுவார்கள். இரத்த கசிவை நிறுத்தாமல் ஏன் அறுவை சிகிச்சை என்று நோயாளியின் உறவினர்கள் குழம்புவார்கள்
இந்த குழப்பங்களுக்கு காரணம் என்னவென்றால் இந்த பிரச்சனையின் தன்மை அப்படி. நோய் என்ன, எதனால், பாதிப்பு எவ்வளவு என்று முதல் இரு தினங்கள் யாராலும் கூற முடியாது. அனைத்து பரிசோதனைகளையும் செய்த பிறகு தான் தெளிவு வரும்.
அதற்குள் மூன்று நான்கு மருத்துவமனை மாற்றினால் சிக்கல்கள் அதிகரிக்கவே செய்யும்
Ma Tholkappiyanனின் ‘லியோ’ – காட்சிமா விமர்சனமும் போலி ஏமாற்று சித்த மருத்துவமும்
அதை சற்றே மாற்றியதில் கீழ்க்கண்ட பதிவு கிடைத்தது. . .
லியோ’ – காட்சிமா விமர்சனம்
“”””””””””””””””””””””””””””
எப்போதெல்லாம் ஒருவர் திடீரென புகழப்படுகிறாரோ அவர் ஒரு போலி என்று கண்டுகொள்க.
எப்போதெல்லாம் ஒரு போலி, ஊடகங்களாலும், பெரும் பணம் படைத்தவர்களாலும், பெரும்பான்மையான சாமானியர்களாலும் கொண்டாடப்படுகிறாரோ அப்போது அவர் ஒரு மாஃபியா ஆகிறார் என்பதை அறிக
இத்தகைய மாஃபியாவாக உருவாக்கப்பட்டவர்தான் லோகேஷ் கனகராஜ். ஏ“மாற்று” சித்த மருத்துவர்
ஓர் அறிவுஜீவியை யாராலும் உருவாக்கமுடியாது; ஒரு காட்சிமா கலைஞனை யாராலும் உருவாக்க முடியாது; ஒரு ஆற்றல் மிக்க கலைஞனை யாராலும் எப்போதும் உருவாக்க முடியாது.
ஆனால், ஒரு முட்டாளை மூளைக்காரனாக காட்ட ஒரு தயாரிப்புஊடக நிறுவனம் வந்து நிற்கும்; ஒரு போலியை அசலாகக் காட்ட ஒரு நாயக நடிகன் முன் வருவான்; ஒரு அறிவிலியை அறிவாளியாகக் காட்ட ஊடகங்கள் ஓடி வரும்.
அவ்வாறு ஊதிப் பெருக்கப்பட்ட முட்டாள்தான்கில்லாடிதான்லோகேஷ் கனகராஜ்.ஏ“மாற்று” சித்த மருத்துவர்
பணம் பிடுங்குவதே மாஃபியாக்களின் ஒரே நோக்கம். பெரும் பணம் பிடுங்க வேண்டும்.
நியாயம் அநியாயம், நேர்மை நீதி, மானம் மனிதாபிமானம், சூடு சொரணை, இரக்கம் கழிவிரக்கம் எவை குறித்தும் கவலைப் படாமல், மக்களை ஏமாற்றி தியேட்டரைஏ“மாற்று” சித்த மருத்துவத்தை நோக்கி அவர்களை இழுத்து வரும் திறமை ஒருவனிடம் இருப்பதாகக் கண்டு பிடித்துவிட்டால், அப்போது அவன்தான் மாஃபியா எனும் அந்தஸ்த்தை பிடிக்கிறான்.
போலி சித்த மருந்து தயாரிப்பாளனுக்கும், நடிகனுக்கும் அதை வைத்து டெண்டர் எடுப்பவருக்கும் பெரும் பணத்தை ஈட்டித் தரும் மாஃபியாதான் லோகேஷ் கனகராஜ். ஏ“மாற்று” சித்த மருத்துவர்
பெரும் பணத்தை மக்களிடமிருந்து கரப்பதால் மட்டுமே ஒருவன் மாஃபியா ஆகிவிடுவது இல்லை. அவன் கல்நெஞ்சக்காரனாகவும் இருக்க வேண்டும். அப்போதுதான் அவன் உண்மையான மாஃபியா ஆக முடியும்.
அதாவது, மக்களை ஏமாற்றி, எத்தகைய சில்லரை வழிகளிலேனும் அவர்களின் ஆசையைத் தூண்டி, அவர்களிடம் இருந்து பணத்தை கரக்கும் ஒரு மாஃபியா, அந்த மக்களுக்கு என்ன கொடுத்தோம் என்று கிஞ்சித்தும் யோசிக்கக் கூடாது. அப்படி யோசிக்காததனால்தான் அவன் மாஃபியா என்று பெருமையாக கொண்டாடப்படுகிறான்.
மக்களின் நேரத்தை அபகரிக்க வேண்டும்; மக்களின் பணத்தை கொள்ளையடிக்க வேண்டும்; கூடுதலாக, மக்களின் மன நிலையை சிதைக்க வேண்டும். இதுதான் மாஃபியாவின் அடிப்படை வேலைத் திட்டம்.
ஒரு காட்சிமா இயக்குநர் ஏ“மாற்று” சித்த மருத்துவர் ஒரு புகழ்பெற்ற மாஃபியாவாக திகழ வேண்டுமானால், அவரிடம் இருக்க வேண்டிய தகுதிகள்,
1.அவனுக்கு கதைமருத்துவம் குறித்த அறிவு இருக்கக் கூடாது.
2.அவனுக்கு பாத்திர வடிவமைப்புப்உடலியங்கியல் பற்றிய அடிப்படைப் புரிதல் தெரியக் கூடாது.
3.காட்சியம்(screenplay)பக்கவிளைவுகள் பற்றிய அறிவோ தெளிவோ கூடவே கூடாது.
4.லாஜிக்கல் பற்றிய கவலையே அவனுக்கு இருக்கக் கூடாது.
ஆனால், முக்கியமான ஒரு புரிதல் அவனுக்கு நிச்சயம் இருக்க வேண்டும். அதாவது,
5.இளைய சமூகத்திடம் இருக்கும் அறியாமைகளையும், மூட நம்பிக்கைகளையும் நன்றாகப் புரிந்து வைத்து இருக்க வேண்டும்.
இந்த ஐந்து அம்சங்களையும் கொண்டிருப்பவன் இந்தச் சமூகத்தின் மரண மாஃபியா ஆகிறான்.
பெரிய பிஸ்தா என்று போற்றப்படுகிற இந்த சினிமாசித்த மாஃபியாவிடம் சொந்தமாக ஒரு கதைமருந்து கூட இல்லை என்று நினைக்கும்போது என்ன சொல்ல!
The History of Violence எனும் ஆங்கிலப்படத்தைடெங்கு, டயாபடிஸ், கோவிட், ஏய்ட்ஸ் ஆகியவற்றிற்கு நவீன அறிவியலின் அடிப்படையில் உள்ள பரிசோதனைகளை அப்படியே தனது முதல் பாதியில் பயன்படுத்தி இருக்கிறான், இந்த மாஃபியா. ஏண்டா அடுத்தவன் பெத்த குழந்தைக்கு எப்டிடா உன்னோட பேற போட்டுக்கிற? கொஞ்சனாச்சும் வெக்கம் மானம், சூடு சொரணை இருக்காடா….? கொஞ்சனாச்சும் முயற்சி பண்ன மாட்டியாடா? ஊரு பணத்தை கொள்ளையடிக்கிறதுல ஒனக்கு கண்ணமுன்ன தெரியாத ஆர்வமாடா?
சமூகம் எப்போதுமே திறமைசாலிகளை கண்டுகொள்வது இல்லை. கண்டுகொண்டாலும் அவர்களுக்கு எளிதில் வரவேற்பு கொடுப்பது இல்லை. ஆனால் எதிர்திறனாலிகள்(inabilitants) உடனடி வரவேற்பை பெற்று விடுகின்றனர்.
யார் இவர்களுக்கு வரவேற்பு கொடுப்பது? லாஜிக்அறிவியல் பற்றி நாம் பேசினால்,,, //சார் லாஜிக்கெல்லாம்அறிவியலெல்லாம் பாத்தா படம் எடுக்கவேவைத்தியம் பார்க்கவே முடியாதுங்க//… என்று நம்மை மறுதலிக்கிறார்கள் பாருங்கள் அவர்கள்தான் போலிகளுக்கு வணக்கமும் வந்தனமும் செய்பவர்கள். வேறு யாருமல்ல.
சமீபத்தில் ஒரு படம்… ‘இருகப்பற்று’ இந்தப் படத்தில் வரும் ஏதேனும் ஒரு காட்சி பார்வையாளனுக்கு பயன் அளிப்பதைப்போல, ‘லியோ’ என்கிற முழுபடத்தாலும் கொடுக்க முடியாது.
அதாவது,
மாஃபியாக்களால் சாமானியனுக்கு ஒரு பொடலங்காய்கூட வேகாது!
ஏமாற்றுக்காரர்களின் சூழ்ச்சிகளில் எனது தமிழ் மக்கள் எளிதில் சுருண்டு விடுகிறார்களே என்று நினைக்கும்போதுதான் இந்த மாஃபியாக்கள் மீது சகித்துக்கொள்ள முடியாத ஆத்திரம் வருகிறது.
என்ன செய்ய! வாய்ப்புக்காகக் காத்திருப்பதைத்தவிர எனக்கு வேறு வழியே இல்லை ம.தொல்காப்பியன்.
Why people who promote 8 years to watch porn needs to be opposed
She is a fraud (as seen from her interviews and social media posts)
Hence she has to be opposed
As simple as that
1. Agree that she is fraud. But Others may be genuine. Why all these Non Medico Influencer’s have to be opposed
They comes with few expected side effects (adverse reactions) and few potential risks
Expected Side effects (adverse reactions) are
Their Knowledge is Limited and many don’t have read more than 20000 words on that topic (50 pages of A4)
Their Confidence is very high and many are on the Peak of Mount Stupid in Dunning Kruger Effect
They not just talk on what they have read (assuming that what they have read is from good sources and not garbage) they also answer with extremely high confidence when asked a related question (about a topic they have not read) and patients get wrong impression
The money being spent on them leads to less money being spent on essential items like Doctor’s Consultation, Drugs, Lab Tests etc
The Potential Risks are
They can promote unwanted items like Cerelac (or such equivalent items)
They can oppose vaccines
They can oppose Institutional Deliveries
They can promote Home Deliveries
The first example costs just money, but the other examples cost lives
Even the expression “just money” has to be used with a pinch of salt because the problem in Indian Healthcare is lack of money to pay to doctors, nurses, drugs, food, equipment and not shortage of doctors, nurses, drugs, food, equipment. Hence any unwanted expense cannot be just brushed under the carpet as “costing money alone”. Anything that costs money in due course costs leads to lack of adequate consultation, nursing care, drugs, diets, equipments all of which are needed
2. Don’t our practices need change? Why not adopt new means and adapt to new means?
Of course, Our Practices do change and we need to adopt new means and adapt to new means. But this change in protocols and practices must be done carefully.
You don’t introduce a new drug without doing studies
But when it comes to introducing protocols, they are done and whims and fancies in the past 3 decades. The expected side effects (adverse reactions) and few potential risks of that scheme / policy / change is not at all taken into consideration.
Those who supported inclusion of healthcare under consumer courts did not think about the expected side effects (adverse reactions) and few potential risks of such act. Those who promoted Clinical Establishment act did not compare expected side effects (adverse reactions) and few potential risks with what they are trying to achieve
Same way, when you want a lactation consultant, Parenting Coach etc, you need to look into what all these can bring to the society in general and healthcare delivery in particular
Merely promoting these with a short sighted views or because few of such people are your personal friends will be wrong
3. The Time Spent per patient by a doctor in a Govt PHC / GH is less. Not all can be told in that limited time? Why not appoint the influencers and pay them?
The Time Spent per patient by a doctors in a Govt PHC / GH is less because there are less doctors and more patients.
There are less doctors because govt does not have money to appoint more doctors
In this case, from where do you have money to appoint a lactation consultant who will look only after lactation.
You can appoint a nurse / doctor in that money and they will be helpful to a larger sector of patients
4. Even in Private Doctors don’t explain for 30 minutes. What is wrong in paying Rs 3000 to this influencer
Pay this Rs 3000 to the Paediatrician and he/she will explain for 30 minutes. Why is that you are not ready and willing to pay Rs 3000 to a Paediatrician for 30 minutes of his / her time, but want to pay a Quack the same amount. Think Think Think
5. Don’t we need More Empathy in Indian Healthcare than we have at present ?
Yes We need. But in any relationship, Empathy has to work both ways. Doctor has to feel for that patient and patient has to feel for the doctor and patient has to also feel for other patients. That is what is called Empathy
If Patient demands doctor to spend 45 minutes with him / her and “suck away” the time to be spent for other patients or “suck away” the time to be spent by the doctor for other purposes, that is not Empathy. It is Exploitation
I have been hearing this word, empathy for the past few years in healthcare. But in every context I have heard it or seen it is actually an demand for exploitation which comes cloaked with empathy.
Next time, you hear this word, pause, think, check whether what is demanded is empathy or exploitation and remember to tell me what you learnt.
6. What is Ego Massage
Ego Massage is defined as the act of spending scarce resources and money are recurrent and non recurrent expenditure which has no benefit in treatment process, but just satisfies the overbloated and useless ego of a patient and / or his relative
7. I have so many problems with our healthcare system. I suggest improvements. But you shoot down my ideas. Don’t you want to improve ?
The problems with our healthcare system are plenty. But 99.99 % of that is due to lack of money. Let me repeat. We don’t lack doctors. We don’t lack nurses. We don’t lack lab technicians. We don’t lack OT Technicians. We don’t lack EEG Technicians. We don’t lack Radiographers. We don’t lack Equipments. We don’t lack skills or raw materials to build a building. We don’t lack drugs. We don’t lack raw materials for drugs. We don’t lack consumables.
But what we lack is the money and willingness to spend money
We lack the money and willingness to pay the doctors
We lack the money and willingness to pay the nurses
We lack the money and willingness to pay the lab technicians
We lack the money and willingness to pay the OT Technicians
We lack the money and willingness to pay the EEG Technicians
We lack the money and willingness to pay the Radiographers
We lack the money and willingness to pay for the Equipments
We lack the money and willingness to pay for the Builing
We lack the money and willingness to pay for the drugs
We lack the money and willingness to pay for the consumables
So, bottom line is : When the problem is due to lack of money, suggesting a costly solution will aggravate the problem and not solve it. Your ideas are shot down immediately because implementing them will cost more money and increase the problems and we will have more problems than we have now.
8. What is wrong in spending more money ?
We can spend only what we earn. If TN GDP is 15 lakhs Crores per year, you cannot spend more than 90 thousand crores (or 6 percentage for health). If the Total Govt Expenditure is 3 lakhs crores per year, you cannot spend more than 18000 crores per year for Govt Institutions
If you are spending more, it means that you are going to spend less for some other department like Education, Roads, Agriculture etc and that is going to be a bigger disaster in due course
So
What you should
Step 1 : Know how much money you have
Step 2 : Device protocols based on that
As per the current GDP, when we don’t have money for having more ambulances or having more Cath Labs or having more Theatres or more blood banks, spending money for Lactation Consultants is a strict no no
9. We have health insurance. Our Company Pay our Insurance Premium. Why not have lactation consultant being paid under insurance?
Before Answering this, I will ask you to check this yourself
How was Detroit in 1990
How is Detroit today
If you have checked you will find that Detroit was one of the richest cities of USA in 1990 and today it is one of the poorest cities. What happened in Detroit is a case study for doctors and especially those who support Health Insurance, Consumer Courts, Ratings etc
Detroit had lots of car factories (Remember that Chennai is called Detroit of Asia) and had one of the largest populations under Regular Employment and hence most people were covered by Health Insurance being paid by the Employer (aka Car Factories). Because it was totally paid by the employer (of course that is a part of salary, but employees did not realise it as it was deducted at source)
And many hospitals got established there and they were over charging the patients. Because many or workers in industries, many occupational diseases were common and for these hospitals were over charging.
They made protocols by whims and fancies
Increased cost of Health care
Increased the Insurance Premium
Seeing this, the insurance companies raised the premium for car workers and the premium kept on increasing and at one stage, the salary (Insurance premium + Take Home) increased so much that it was not profitable to make cars in Detroit
Detroit Today
That is how Chennai became Detroit of Asia
Demanding Luxury in healthcare is a sure way to ensure that you don’t get the mandatory healthcare.
10. What I demand is basic. It is not luxury. How dare you call it luxury?
As explained above, what is basic and what is luxury can be determined based on the GDP of that Family / Street / Town / State / Country and not based on the individual’s whims and fancies.
Assume you earn 2 lakhs per month. You can travel by 3AC. But some one who earns 40000 per month can travel by SL only. Now, what happens when you make all coaches as 3AC. Two problems will happen
The 3AC coaches will not be full
One who cannot afford this will have to walk instead of train
In long run, since the 3AC coaches are not full, the train will be stopped. Same way, when you demand luxury in healthcare, hospitals will be forced to close in due course. Just like what happened to the hospitals in Detroit.
Why Do So Call Health Conscious People who go to Gym Daily and Do Proper Exercises Get Heart Attack and that too at younger Age ?
Should we go to Gym or Not ?
Let us see
-oOo-
Consciousness and Awareness have different meanings when used as Adjective
For example
Health Conscious – Means Knowing the importance of maintaining Good Health and doing somethingfor that
Health Awareness – Means Means Knowing the importance of maintaining Good Health and doing the right thingfor it
-oOo-
Those who don’t mind about the health are not health conscious. Examples are those who don’t know what is their Blood Sugar and Blood Pressure
Those who mind about their health, but do the wrong things are health-conscious, but not health-aware. These are people who know about diabetes, have checked their blood sugar and found that they have diabetes, but read “Organic Eugenics” books and watch such videos and eat millets and jaggery and pay lots of money for “Chekku” Oil
Those who mind about their health, but do the correct things are health-conscious as well as health-aware. These are people who know about diabetes, have checked their blood sugar and follow scientific methods to improve their health
-oOo-
The common factor behind diseases like Heart Attack, Stroke, Vision Problems, Kidney Failure etc is clogging of blood vessels.
This clogging of blood vessels is due to
(I)
Damage to the inner wall of the blood vessels. (Scientifically it is called Endothelial Damage)
(II)
Increased Clot Forming Ability
-oOo-
(I)
This damage to the inner wall happens because of various reasons
(I.A) Structurally Weak Inner Wall
1. Those whose inner wall is weak due to various Genes. In these people, even a normal blood sugar and normal blood pressure cause more damage
(I.B) Damage Due to Mechanical Reasons
2. High Blood Pressure. Your Blood Vessels are like Pipes or Garden Hoses. What happens when the pressure of water flowing in a pipe is high. It gets damaged easily. Isn’t it. Similarly when the blood pressure is high, your blood vessel’s inner wall get damaged soon.
3. High Pulse Rate : What happens when you take a straw and fold it. You will see a damage in the straw. What if you fold again and again. At one point the damage will be severe. Same way, When your blood vessels are bent and unbent again and again, the rate of injury to the inner walls. There are many blood vessels which get bent again and again. The vessels which gets bent maximum times in the one in your heart. It gets bent every time your heart beats. The vessels of your neck gets bent every time you move your neck. The vessels of your knee gets bend every time you move your knee. (This is why atherosclerosis is so common in Coronary, Carotid, Vertebral and Popliteal arteries)
(I.C) Damage Due to Chemical Reasons
Assume few different garden hoses. One in which only water flows. Another in which acid flows. Which will get damaged quicker ?
Same way,
Your blood vessels are also damaged as per what is in the blood
4. High Blood Sugar : Damages the blood vessels and leads to reduced blood flow. This is exactly why we need to keep the blood sugar under control. The damages may not be visible immediately, but they will accumulate
5. High LDL : Just like High Cholesterol, this too damage the blood vessels
6. Free Radicals : also damage the inner wall
7. Hyperhomocysteinemia : Homocysteine is a sulfur amino acid whose metabolism stands at the intersection of two pathways: remethylation to methionine, which requires folate and vitamin B12 (or betaine in an alternative reaction); and transsulfuration to cystathionine, which requires pyridoxal-5′-phosphate. When there is problem in either of these pathways, the level of Homocysteine in the body increases. When it increases beyond a certain level, it causes damages to the inner wall of the blood vessels causing reduction in blood flow.
(II) Increased Clot Forming Ability : Hope you know the disease Hemophilia. This is a condition where blood does not clot easily. There are lots of diseases where the other end happens. That is Blood clots easily. In such cases, the person is at risk of developing clot even when Blood Sugar, Pressure, Cholesterol levels are normal. And the most important part is these conditions cannot be solved by exercise, walking etc
Increased Clot Forming Ability can be due to
(II.A) Congenital / Inborn : These are due to reasons where the individual has few genes which increase the clot forming ability of blood
8. Factor V Leiden and Prothrombin G2021A mutation.
9. Antithrombin III, protein C and protein S deficiency
So
Whether you will get a heart attack (or stroke or kidney failure or vision problem or neuropathy) depends on so many factors
And
You need evaluate and manage accordingly
-oOo-
So
1. You get heart attack if your vessels are weak from birth due to your genes
2. You get heart attack if your BP is high
3. You get heart attack if your Pulse is high
4. You get heart attack if your blood sugar is high
5. You get heart attack if your LDL is high (please don’t get fooled by half baked idiots who say that LDL is not an issue)
6. You get heart attack if Free Radicals are high in your body
7. You get heart attack if there is homocysteinaemia
8. You get heart attack if you have Factor V Leiden and Prothrombin G2021A mutation. (Please don’t order a test yourself and spend 1000s of rupees and then go an ask the doctor to explain it. It does not work that way)
9. You get heart attack if you have Antithrombin III, protein C and protein S deficiency
10. You get heart attack if you undergo Surgery,
11. You get heart attack if you are Pregnant and have other heart issues
12. You get heart attack if you undergo Hormonal replacement therapy,
13. You get heart attack if you use Hormonal Contraception (Condoms are the safest)
14. You get heart attack if you have cancer (malignancy)
15. You get heart attack if you have Inflammation,
16. You get heart attack during or after Infection eg Post COVID 19 Thrombosis
-oOo-
So there are multiple factors
I have listed just a few
There are many others too
-oOo-
So Treatment to prevent Heart Attack (or other such complications) has to be a multi pronged approach.
Exercise and Diet are the first line of approach But at the same time, you need to understand that mere Exercise won’t help and Mere Diet won’t help
-oOo-
Now
What will happen when a person exercises
Heart Rate will increase
BP will increase
What happens when heart rate increases
There is bending and unbending the the blood vessels of heart
What happens when BP increases
There is increased pressure to the inner wall of the blood vessels of heart
What happens when there is bending and unbending and increased pressure There is damage to the inner wall
-oOo-
Now Coming to the Questions
Why Do So Call Health Conscious People who go to Gym Daily and Do Proper Exercises Get Heart Attack and that too at younger Age ?
When you exercise, you damage your inner wall. Now, if there are no other causes for damage to wall and if there are no other causes of increased coagulability at work, there is time for the damages to be repaired
But
When other risk factors (increased sugar, increased LDL, post covid thrombosis) are also present There is no time for the body to repair the damaged inner walls and there is an heart attack
-oOo-
Should we go to Gym or Not ?
Please go to Gym
But Please correct your Blood Sugar, Pulse Rate, Blood Pressure, Hypercoagulability first and then go to Gym
-oOo-
If you have no risk factors –> Gym increases your lifespan
If you have risk factors and have corrected them with diet + drugs –> Gym increases your lifespan
If you have risk factors and you have avoided tablets and think that you can solve all the problems with exercise alone –> Gym REDUCES your lifespan
-oOo-
Moral
1.
Human Body Structures are complex
Human Body Functions are complex
There are multiple factors at play
2.
Don’t follow some advice based on Whatsapp forwards / Facebook Posts / Videos / Instagram Reels. Many of such Videos (including the one by few “doctors” are based on some random articles with scant regard to Physiology, Pathology, Community Health).
3.
When you have risk factors, Tablets plus Gym is Best
When you have risk factors, Tablets alone are better
When you have risk factors, Keeping Quite and Doing nothing is bad
When you have risk factors, Gym without Tablets is giving Friend Request to EmaDharmaRaja and then calling him over phone and asking to accept the request !
-oOo-
Feel free to ask doubts
If you want to know about complications of diabetes and how to prevent them, read this book : Myths and Facts about LCHF (Low Carb High Fat) Diet and “Reversal” of Type 2 Diabetes: How Paleo, Keto, Atkin’s Diets Work https://amzn.to/3VbRcac
Myths and Facts about LCHF (Low Carb High Fat) Diet and “Reversal” of Type 2 Diabetes: How Paleo, Keto, Atkin’s Diets Work
நீரழிவு நோய்க்கு ஏற்ற உணவு குறித்து அறிய : பேலியோ உணவின் அறிவியலும் உளவியலும்: Science and Psychology of Paleo Diet (Tamil Edition) https://amzn.to/3XcZSPw நூலை வாசிக்கவும்
புருனோ Bruno பேலியோ உணவின் அறிவியலும் உளவியலும்: Science and Psychology of Paleo Diet
Comment :
Anti thrombosis therapy for COVID-19 has always been a part of treatment guidelines.
https://www.covid19treatmentguidelines.nih.gov/therapies/antithrombotic-therapy/ It’s high time TN docs follow such validated ones rather than following their own cocktails.
My Response :
They are doing this only during hospital stay and stop it without checking coagulation profile But, I am asking this to be done based on coagulation profile
Use of steroids Was done by us Months before it was added to NIH
By the time they validate, We will lose another lakh
What is wrong in doing coagulation profile and treating that ??
Other than cost, Can you give any reason
Comment :
Use of steroids started because someone saw it being considered in certain trials (Solidarity trial). We ended up using it indiscriminately leading to mucor surge.
My Response :
For decades, We have been using steroids for treating pneumonia
You are answering the question : How to ignore Bruno’s recommendations
I am answering the question : How to save lives
Both are talking entirely different topics
Between The recommendation you have quoted and my recommendations, which can save more lives
Comment :
Evidence based medicine vs Eminence based medicine. What do u prefer ?
If you want to prove something then conduct a study – even a small one – look at the results and communicate widely.
My Response :
I prefer evidence based medicine
I prefer to give anticoagulants based on PT, aPTT, INR and other tests
I don’t prefer eminence based medicine – of quoting NIH guidelines – ignoring basic common sense
That is exactly what I say – Do coagulation profile, Treat as per results
What is wrong in the statement – Do coagulation profile and treat as per results
This is the evidence based medicine
Is it clear boss
Prove what ?
You want proof for the statement “Treat abnormal coagulation profile”
Come on saaar. . . It is 2nd year mbbs stuff
Comment :
Treat abnormal coagulation profile – is part of inpatient management boss – done routinely everywhere
My Response :
Perfect
That is what I am also saying
So
What did you really want me to prove
Comment (quoting my journal article) :
this – the prophylactic part
My Response :
The first statement is Do Coagulation profile for those at risk
The second Statement is Treat abnormal coagulation profile
Which statement are you asking proof ?
Which statement is not evidence based medicine ?
Read again. I never ask to give drugs. I ask to first do tests and give drugs only when results indicate it
What is the problem there ?
கிணற்றில் இருந்து நீரை எடுக்கவேண்டுமென்றால் கயிற்றில் வாளியை கட்டி எடுக்கலாம்.
அல்லது ஓடி (மோட்டார்) மூலம் எடுக்கலாம். அப்படி ஓடி (மோட்டார்) மூலம் எடுக்கும் போது நீர் வர ஒரு குழாய் தேவை. அத்துடன் ஓடிக்கு மின்சாரம் கொண்டு வர கம்பி (வயர்) தேவை
-oOo-
Bruno’s Tweet on Nerve Vein Artery
இதே போல் நமது உடம்பில் சில உறுப்புகள் உள்ளன. எலும்புகளை எலும்புடன் சேர்க்கும் எலும்புநாண் / எலும்புநார் (Ligament)
எலும்புகளை தசையுடன் சேர்க்கும் தசைநார் (Tendon)
இரத்தத்தை கொண்டு சேர்க்கும் இரத்தக்குழாய்கள் (Blood Vessels)
உறுப்புகளில் இருந்து மூளைக்கு செய்திகளை அனுப்பும், மூளையில் இருந்து உறுப்புகளுக்கு செய்திகளை அனுப்பு நரம்புகள் (Nerves)
-oOo-
இதில் இரத்த குழாய்கள் என்பது இருவகைப்படும்
இதயத்தில் இருந்து பிற உறுப்புகளுக்கு இரத்தத்தை கொண்டு செல்லும் தமணிகள் (Arteries)
பிற உறுப்புகளில் இருந்து இதயத்திற்கு இரத்தத்தை கொண்டு செல்லும் சிரைகள் (Veins)
-oOo-
உடலில் நீர்ச்சத்து குறைவாக இருந்தால் நாம் திரவங்களை ஏற்றுகிறோம் அல்லவா. அதற்கு நாம் பயன்படுத்துவது சிரைகளை (Veins). இரத்தம் ஏற்ற வேண்டும் என்றாலும் சிரைகள் மூலம் தான் ஏற்றவேண்டும். அதே போல் ஊசியில் மருந்து செலுத்தும் போதும் சிரைகளில் செலுத்தலாம். இதை சிரை வழி திரவம், (Intravenous Infusion) சிரை வழி ஊசி / சிரையுள் ஊசி, சிரைவழியாக ஊசி, சிரையக ஊசி (Intravenous Injection or IV Injection) என்று அழைப்பார்கள்.
தசைகளில் (தோளில், பிட்டத்தில்) போடப்படும் ஊசி தசையுள் ஊசி (Intra muscular Injection or IM Injection).
தோலுக்கு அடியில் போடப்படும் தோலடி ஊசி (Subcutaneous Injection or SC Injection)
தோலுக்குள் போடப்படும் ஊசியும் உண்டு (Intradermal)
-oOo-
இன்று நாம்
எலும்புநாண் / எலும்புநார்
தசைநாண் / தசைநார்
தமணி
சிரை
நரம்பு
என்று பிரித்து சொன்னாலும்
ஒரு காலத்தில்
இவை அனைத்தையும் நரம்பு என்றே அழைத்தார்கள்.
இந்த பிரச்சனை தமிழில் மட்டுமல்ல, கிரேக்க மொழியிலும், இலத்தீன் மொழியிலும் இதே போல் தான் இருந்துள்ளது
The Greek word neuron was used to designate a tendon, but also a nerve, ligament and vein.
Latin expression nervus designated a muscle, a tendon, a nerve or something formed from tendons (Oxford Latin Dictionary, 1968)
Latin Nervus; Greek Neuron; Tamil Narambu நரம்பு all three used to denote Nerves, Veins, Tendon, Ligament
-oOo-
எனவே சிரைவழி ஊசிகளை நம் மக்கள் நரம்பூசி என்றே அழைத்தனர்.
முன்னோர் தான் முட்டாள் இல்லையே, பிறகு நாம் ஏன் அதை மாற்றவேண்டும், அப்படியே தொடர்ந்து அழைக்கக்கூடாது என்று கேள்வி எழுகிறதா ?
இதற்கு பதில் உள்ளது
சுமார் 100 ஆண்டுகளுக்கு முன்னர் சிரை வழி ஊசிகள் மட்டுமே போடப்பட்டு வந்தன. எனவே நரம்பூசி என்று அழைத்தாலும் கூட அது சிரைக்குள் செலுத்துவதை மட்டுமே குறித்தது.
ஆனால்
அறிவியல் வளர வளர
தமணிக்குள்ளும் ஊசிகளை செலுத்தும் பழக்கம் வந்தது. முக்கியமாக புற்று நோய் சிகிச்சையில் இது 1950களில் இருந்தே பயன்பாட்டில் உள்ளது (Klopp CT, Alford TC, Bateman J, Berry GN, Winship T. Fractionated intra-arterial cancer; chemotherapy with methyl bis amine hydrochloride; a preliminary report. Ann Surg. 1950;132:811–32 & Bonner CD, Thurman A, Homburger F. A critical study of regional intra-arterial nitrogen mustard therapy in cancer. Ann Surg. 1952;136:912–8)
அதே போல்
நரம்புகளை சுற்றி மருந்து செலுத்தும் பழக்கமும் உள்ளது. அறுவை சிகிச்சையின் போது வலி தெரியாமல் இருக்க போடுகிறார்கள் அல்லவா. அந்த ஊசியை நரம்புகளை சுற்றி செலுத்துவார்கள். இதை மரத்து போகும் ஊசி என்றும் அழைப்பார்கள். ஸ்பைனல் அனஸ்தீசியா என்பதும் இந்த வகைதான்
எனவே இன்றைய தேதியில்
நரம்பூசி என்பது வேறு
தமணியுள் ஊசி என்பது வேறு
சிரையுள் ஊசி என்பது வேறு
எனவே
இனியும் சிரைவழி திரவங்களையும், சிரையுள் ஊசியையும் “நரம்பூசி” என்று பொதுவாக அழைப்பதை தவிர்க்கலாமே
-oOo-
நரம்பு துண்டாகி இரத்தப்போக்கு ஏற்பட்டு வாலிபர் பலி என்று இந்த செய்தியில் தவறாக உள்ளது
நரம்பு துண்டாகி இரத்தப்போக்கு ஏற்பட்டு வாலிபர் பலி என்று இந்த செய்தியில் தவறாக உள்ளது
தமணி துண்டாகி அல்லது சிரை துண்டாகி என்று எழுதியிருக்கவேண்டும். தமணியா, சிரையா, எது பிரச்சனை என்று தெரியாவிட்டால் ”இரத்தக்குழாய் துண்டாகி என்று எழுதியிருக்கலாம்” இப்படி எழுதுவது பிழை
1990களில் இந்தியாவில் Hire and Fire நடைமுறை வந்தது. அதன் பிறகு Outsourcing / Contract (ஒப்பந்தப்பணி) ஆகியவை வந்தன
இதன் பின்னால் இருக்கும் முக்கிய காரணி – Technology அல்லது தொழிற்நுட்பம்
-oOo-
முன் காலங்களில் ஒரு வேலையை செய்ய நிறைய திறமை, நிறைய அனுபவம் தேவைப்பட்டது.
அல்லது / மற்றும்
நீண்ட கால அனுபவம் உள்ளவர் செய்வதற்கும், குறுகிய காலம் அனுபவம் உள்ளவர் செய்வதற்கும் வித்தியாசம் நிறைய இருந்தது
எனவே நீண்ட கால அனுபவம் உள்ளவர்கள் தேவைப்பட்டார்கள்.
ஆனால் தொழிற்நுட்பம் வளர வளர,
தேவைப்படும் அனுபவம் குறைந்தது
அல்லது / மற்றும்
நீண்ட கால அனுபவம் உள்ளவர் செய்வதற்கும், குறுகிய காலம் அனுபவம் உள்ளவர் செய்வதற்கும் வித்தியாசம் குறைந்தது
-oOo-
உதாரணமாக மருத்துவமனை மருந்தகத்தில்அந்த காலத்தில் Compounder என்று ஒருவர் இருந்தார். அப்பொழுது மருந்தகத்தில் (Pharmacy) மருந்துகள் செய்யப்பட்டன.
Mixtures, Lininment, Ointment, Cream எல்லாம் அங்கு செய்யப்பட்டன. எனவே அதற்கு அனுபவம் தேவை.
புதிதாக வருபவர் செய்யும் Ointment mixture போல் வரும் ரிஸ்க் இருப்பதால் நிறுவனங்கள் அனுபவம் மிக்க மருந்தாளுனர்களை இழக்க விரும்ப மாட்டார்கள். எனவே நிரந்திர பணி அளித்தார்கள்.
ஆனால் இன்று அனைத்தும் Blister pack, tubeகளில் வருகின்றன. எனவே மருந்தாளுனரின் வேலை என்பது செஷ்பில் இருந்து எடுத்து கொடுப்பது தான். எனவே பணி நிரந்தரம் இல்லை
அதே போல்
முன் காலங்களில் ஆய்வகங்கள் ஒவ்வொரு பரிசோதனையையும் தனியா செய்ய வேண்டும்
இப்பொழுது Semi Auto Analyser வந்து விட்டது. பல பரிசோதனைகள் Card Test / Rapid Kit ஆக வந்து விட்டன.
எனவே அனுபவத்தின் மதிப்பு குறைந்துள்ளது
-oOo-
மலேரியாவை கண்டு பிடிக்கும் ஆய்வக நுட்பனர் பணி என்பது நிரந்தர பணியாக உள்ளது. காரணம் இது அனுபவம் தேவைப்படும் வேலை
எய்ட்ஸ் சிகிச்சை பிரிவில் இருக்கும் ஆய்வக உதவியாளர் ஒப்பந்த பணியில் உள்ளார். இது சில நாட்கள் பயிற்சி பெற்றால் போதும்
-oOo-
ஒப்பந்த பணியால் வேறு பல பிரச்சனைகள் உள்ளன. அதை நான் முழுவதும் ஆதரிக்கவில்லை. அது வேறு விஷயம் – அது குறித்து தனியாக பேசலாம்
இங்கு கூறவரும் விஷயம் என்னவென்றால்
When technology has replaced your skill, you have lost your bargaining power
-oOo-
1990கள் வரை நிறுவனங்களின் இன்றியமையாத பங்காக தட்டச்சர்கள் இருந்தார்கள். ஏன் ? நிறைய கடிதங்களை விரைவாக அடிக்கவேண்டும். தவறில்லாமல் அடிக்கவேண்டும்
ஆனால் கணினி வந்த பிறகு தவறுகளை திருத்தும் வாய்ப்பு வந்த பிறகு “தவறில்லாமல் அடிப்பது” என்ற திறமைக்கு மதிப்பில்லை
-oOo-
சுவரில் படம் வரைபவர்களின் வேலையை போட்டோஷாப் + கோரல்டிரா + ப்ளெக்ஸ் பிரிண்டிங் பறித்தது
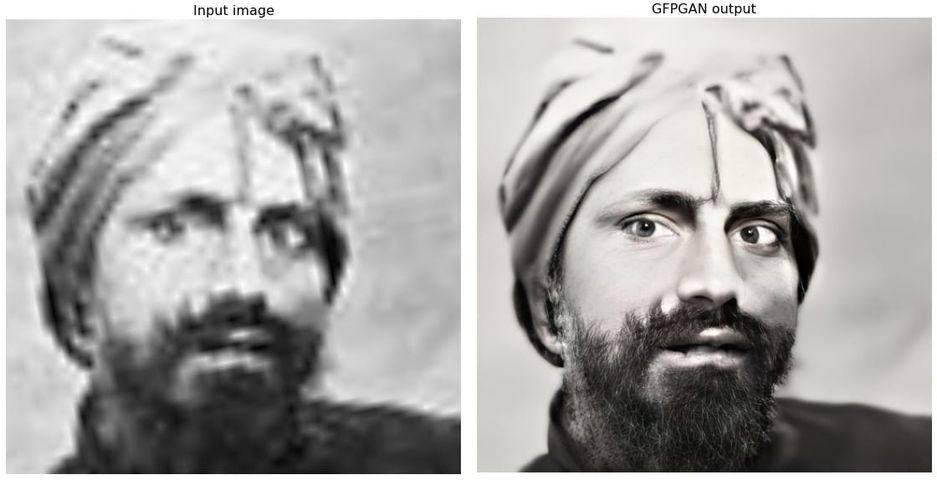
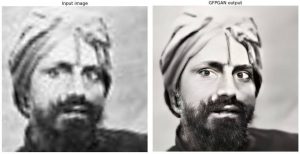
செயற்கை நுண்ணறிவு வந்து பழைய படத்தை சீரமைக்கும் திறமை சாலிகளின் வேலையை பறிக்கும். இந்த படத்தை பாருங்கள்.
(மூலம் : https://www.facebook.com/chithranraghu/posts/10227921004110055
மென்பொருள் : https://github.com/TencentARC/GFPGAN & https://replicate.com/xinntao/gfpgan)
2000களின் ஆரம்பம் முதல் இன்று வரை மிக அதிகமாக தேவைப்படும் ஒரு திறமை (பழைய படங்களை புதுப்பிற்பது) இனி பின்னால் சென்று விடும்
-oOo-
எனவே
நிரந்தர பணி x ஒப்பந்தப்பணி
குறித்த உரையாடல்களில்
உலகவங்கி, காட் என்று மட்டும் ஜல்லியடித்துவிட்டு
தொழிற்நுட்பத்தின் பங்கு குறித்து பேசவில்லை என்றால்
அது முழுமையாகாது
-oOo-
இந்தியாவில் கம்யூனிஸ்ட் கட்சி தொழிற்சங்கம் இருக்கும் தொழிற்சாலைகள் உருப்படுவதில்லை
காங்கிரஸ், திமுக தொழிற்சங்கங்கள் பலமாக இருக்கும் தொழிற்சாலைகள் தப்பிக்கின்றன
காரணம் என்ன தெரியுமா ?
-oOo-
இதற்கு செல்லவதற்கு முன்னர் இந்த கோப்பை வாசியுங்கள்
சிகிச்சையில் முக்கியம்
1. அந்த சிகிச்சை இருக்கவேண்டும்
2. அந்த சிகிச்சை நம் அருகில் இருக்கவேண்டும்
3. அந்த சிகிச்சை நம் அருகில், நம்மால் வாங்கக்கூடிய விலையில் இருக்கவேண்டும்
4. அந்த சிகிச்சை நம் அருகில், நம்மால் வாங்கக்கூடிய விலையில், தரத்துடன் இருக்கவேண்டும்
இதில் முதலில் தேவை – இருப்பது
அடுத்த முக்கியம் – அருகில் இருப்பது
அடுத்த முக்கியம் – வாங்கும் விலையில் இருப்பது
அடுத்த முக்கியம் – தரமாக இருப்பது
மிக அதிகமான தரமாக உள்ளது, ஆனால் வாங்கும் விலையில் இல்லை என்றால் பலனில்லை
மிக அதிகமான தரமாக உள்ளது, ஆனால் அருகில் இல்லை என்றால் பலனில்லை
எனவே எப்பொழுதும் Order of Priority முக்கியம்
-oOo-
ஊதியம் அவசியம்
அதை விட தொழிலாளர் நலன் அவசியம்
இவர் இரண்டும் எப்பொழுது அவசியம் ?
அந்த தொழிலாளி வேலையில் இருந்தால் தானே இவை இரண்டிற்கும் அர்த்தம் உண்டு
வேலையில் இல்லை என்றால் அதிக ஊதியம் என்ற கோரிக்கையால் ஏதாவது பலன் உண்டா ?
தொழிலாளி வேலையில் இருக்கவேண்டும் என்றால் எது அவசியம் ?
தொழிலாளி வேலையில் இருக்கவேண்டும் என்றால் அந்த தொழிற்சாலை, நிறுவனம் இயங்கவேண்டும்
எனவே
முதல் தேவை – தொழிற்சாலை இயங்கவேண்டும்
அடுத்த தேவை – நமக்கு (தொழிலாளிக்கு) வேலை வேண்டும்
அடுத்த தேவை – நமது அடிப்படை உரிமை + பாதுகாப்பு வேண்டும்
அடுத்த தேவை – ஊதிய உயர்வு வேண்டும்
-oOo-
காங்கிரஸ், திமுக தொழிற்சங்கங்கள் இந்த கருத்தில் தெளிவாக இருப்பார்கள்
ஊழியரின் உடல் நலத்திற்கோ, உயிருக்கு ஆபத்து என்ற நிலை எற்பட்டால் தவிர அவர்கள் வேலை நிறுத்தத்தில் ஈடு படமாட்டார்கள்
மீதி பிரச்சனைகளை ”பேசியே தீர்த்துக்கொள்வார்கள்”
லாக் அவுட் போன்ற விஷயங்களினால் தொழிற்சாலைக்கு நஷ்டம் என்றால் அது ஊழியர்களை பாதிக்கும் என்பதில் அவர்கள் தெளிவாக இருப்பார்கள்
-oOo-
கம்யூனிஸ்ட் தொழிற்சங்கங்களை பொருத்தவரை
அவர்களுக்கு போராட்டம் தேவை
அதனால் ஊழியருக்கு வேலை போனாலும் பரவாயில்லை (விடுங்க பாஸ், கோர்ட்டில் போய் வாங்கிக்கலாம்)
அதனால் தொழிற்சாலை இழுத்து மூடப்பட்டாலும் பரவாயில்லை (விடுங்க பாஸ், லேபர் டிபார்ட்மெண்டில் பேசி செட்டில்மெண்ட் வாங்கலாம்)
என்று தான் இவர்களின் செயல்பாடு இருக்குமே தவிர
அவர்கள் சங்கம் வளர்ப்பது தான் அவர்களின் நோக்கமாக இருக்கும் தவிர
ஊழியர் நலன் துளியும் இருக்காது
இது தான் என் அனுபவம்
-oOo-
ஆமை புகுந்த வீடும்
கம்யூனிஸ்ட் புகுந்த தொழிற்சாலையும்
உருப்பட்டதாக சரித்திரமே இல்லை
ஒருவருக்கு பைல்ஸ் பிரச்சனை அல்லது சிறுநீரக கோளாறு இருக்கிறது என்று வைத்துக்கொள்ளுங்கள்.
இப்பொழுது அவர் வைத்தியம் செய்து கொள்ள நிறைய இடங்கள் உள்ளன
1. அரசு மருத்துவமனையில் – இலவசமாக
2. தனியார் மருத்துவமனையில் – காசு கட்டி
3. தனியார் மருத்துவமனையில் – காப்பீடு மூலம் (அதாவது ஏற்கனவே காப்பீடு திட்டத்தில் சேர்ந்திருந்தால்)
எந்த மருத்துவமனை செல்வது என்பதை தீர்மானிக்க அவருக்கும் அவரது குடும்பத்தினருக்கும் நேரம் உள்ளது.
அவர் தனியார் மருத்துவமனையில் சேர்கிறார் என்றால், அவர் பணம் கட்டுவார் அல்லது அவரது காப்பீடு திட்டத்தை வைத்து அந்த மருத்துவமனை காப்பீடு நிறுவனத்திற்கு விண்ணப்பிப்பார்கள். அப்படி விண்ணப்பித்தவுடன், அந்த நிறுவனம் அதை அங்கீகரிக்கும். அதை வைத்து சிகிச்சை துவங்கும்
அவசரமில்லாத சிகிச்சைகளுக்கு இந்த பிரச்சனை இல்லை ஆனால் விபத்துக்களில் சிக்கல் உள்ளது
-oOo-
அடி சிறிது என்றால் – சிராய்ப்பு மட்டும் தான் என்றால்- முதலுதவி சிறிது தான், சிகிச்சையும் சிறிது தான்.
ஆனால் அடி பலம் என்றால் – தலைக்காயம் அல்லது விலா எலும்பு முறிவு, கை கால் எலும்பு முறிவு என்றால்- முதலுதவியும் அதிகம், சிகிச்சையும் அதிகம்.
உதாரணமாக,
சிராய்ப்பு என்றால் முதலுதவிக்கு 100 ரூபாய் ஆகும். மொத்த வைத்தியம் ரூ500 முதல் ரூ1000 வரை ஆகும்.
கை எலும்பு முறிவு என்றால் முதலுதவிக்கு 1000 ரூபாய் ஆகும். மொத்த வைத்தியம் ரூ10000-ரூ30000 வரை ஆகலாம்.
கால் எலும்பு முறிவு என்றால் முதலுதவிக்கு 10000 ரூபாய் ஆகும். மொத்த வைத்தியம் ரூ1 லட்சம் – ரூ2 லட்சம் வரை ஆகலாம்.
தலைக்காயம் / முதுகு எலும்பு முறிவு என்றால் முதலுதவிக்கே ரூ1 லட்சம் ஆகும். மொத்த கட்டணம் ரூ3 லட்சம் முதல் ரூ10 லட்சம் ஆகலாம்
இது புரிந்து கொள்ளத்தான். சரியான கட்டணம் என்பது நபருக்கு நபர் மாறுபடும்.
-oOo-
முதலுதவிக்கு 1 லட்சமா என்று கேள்வி எழுகிறதா ?
1980களில் முதலுதவி என்பது கட்டு போடுவது + வலிக்கு மாத்திரை அளிப்பது மட்டுமே. 1980களில் முதலுதவி என்பதை ஒரு சிறிய பெட்டிக்குள் அடக்கி விடலாம்
2021ல் முதலுதவி என்பதே பெரிதாகிவிட்டது
Philadelphia Collar / Spine Board / Pelvic Binders / Splints
Suction / OP Airway / NP Airway / Intubation / Tracheostomy
Ventilatory Suppor
Venflon / Central Line
Stat Lab
Volume Replacement Blood Transfusion
X Ray / eFast / CT / MRI
ICD / Pericardiocentesis
எனவே இன்றைய தேதிக்கு
உண்மையான முதலுதவி என்பது விபத்தின் தன்மையை பொருத்து 10 ரூபாயில் இருந்து (சிராய்ப்பு என்றால்) ரூ1 லட்சம் வரை (தலைக்காயம் + எலும்பு முறிவு + நுரையீரல் பாதிப்பு) ஆகும்.
-oOo-
சும்மா ஒரு கட்டு போட்டுவிட்டு, டிடி ஊசி போடுவது என்றால் 100 ரூபாய் செலவு. ஆனால் உண்மையில் உயிரை காக்க வேண்டும் என்றால் 1 லட்சம் செலவு.
சும்மா ஒரு கட்டு போட்டுவிட்டு, டிடி ஊசி போடுவது என்றால் 10 நிமிடம் தான் ஆகும். ஆனால் உண்மையில் உயிரை காக்க வேண்டும் என்றால் 6 மணி நேரம் வரை ஆகலாம்.
-oOo-
அந்த காலத்தில் எல்லாம் அடிபட்டால் 10 ரூபாய் தான் செலவு. இப்ப 1 லட்சமா, ஹாஸ்பிட்டல் எல்லாம் கொள்ளையடிக்கிறாங்க என்று புலம்புகிறீர்களா ?
சற்றுப் பொறுங்கள்.
விபத்தினால் நேரும் மரணங்களை கீழ்க்கண்டவாறு பகுக்கலாம்.
(1) முதல் வகை: மூளை, இதயம், மகாதமணி, முதுகுத்தண்டு ஆகியவை கிழிபடுவதால் ஏற்படும் உடனடி மரணம் – இது அடிபட்ட சில நொடிகளில் இருந்து 10 நிமிடங்களுக்குள் ஏற்படும். இதில் உயிரை காக்க வாய்ப்பு குறைவு. விபத்தை தடுப்பதன் மூலமே இதை தடுக்க முடியும்.
(2) இரண்டாம் வகை : மண்டக்குள் இரத்தக்கட்டு, நுரையீரலை சுற்றி இரத்தம் கட்டுவது, இதயத்தை சுற்றி இரத்தம் கட்டுவது, இரத்தப்போக்கு, மூச்சுத் திணறல் ஆகியவற்றால் ஏற்படும் மரணங்கள். இவை 10 நிமிடங்களில் இருந்து 2-3 நாட்களுக்குள் ஏற்படும். ஆனால் அடிபட்ட உடனே, அடிபட்ட 1 மணி நேரத்திற்குள் சிகிச்சையை அளிப்பதன் மூலம் இவர்களின் உயிரை காக்க முடியும்.
(3) மூன்றால் வகை : பிற அடிகள்.
-oOo-
1980களில் முதலுதவி என்பது கட்டு போடுவது + வலிக்கு மாத்திரை அளிப்பது மட்டுமே. 1980களில் முதலுதவி என்பதை ஒரு சிறிய பெட்டிக்குள் அடக்கி விடலாம். காரணம் அன்றைய காலக்கட்டத்தில் நாம் மூன்றாம் வகை அடிகளுக்கு மட்டும் தான் முதலுதவி செய்து வந்தோம்.
அன்றைய காலக்கட்டத்தில்
மண்டைக்குள் இரத்தக்கட்டு, நுரையீரலை சுற்றி இரத்தம் கட்டுவது, இதயத்தை சுற்றி இரத்தம் கட்டுவது, இரத்தப்போக்கு, மூச்சு திணறல் ஏற்பட்டால் மரணம் தான்.
அதாவது 1980களை பொருத்தவரை,
முதல் வகை + இரண்டாம் வகை இரண்டுமே ஸ்பாட் அவுட் தான்
ஆனால் 2021ல் நவீன அறிவியல் மருத்துவம் வளர்ந்த பிறகு இரண்டாம் வகைக்கு சிகிச்சை வந்துள்ளது. அதன் மூலம் உயிரை காக்க முடிகிறது. ஆனால் இதற்கு ரூ3 லட்சம் முதல் 10 லட்சம் வரை ஆகிறது. இந்த முதலுதவிக்கே ரூ1 லட்சம் ஆகிறது
அந்த காலத்தில் அடி பட்டு “ஸ்பாட் அவுட்” என்று கணக்கில் வந்தவர்களில் பாதி பேரை காக்க முதலுதவிக்கே 1 லட்சம் ஆகிறது.
அதாவது 10 ரூபாய் கட்டு போதுவது 1 லட்சம் ஆகவில்லை, புதிதாக 1 லட்சத்திற்கு சிகிச்சை வந்துள்ளது.
-oOo-
ஒருவர் சாலையில் செல்லும் போது விபத்துக்காகிறார் என்றால், அவர் கையில் 1 லட்சம் இருந்தால் அவருக்கு தனியார் மருத்துவமனையில் சிகிச்சை அளிப்பதில் எந்த பிரச்சனையும் இல்லை.
அவர் கையில் காசு இல்லை என்றால் அந்த தனியார் மருத்துவமனைக்கு யார் காசு கொடுப்பார்கள்?
அவர் கையில் காசு இல்லை, ஆனால் அவரிடம் காப்பீடு உள்ளது. அந்த காப்பீடு எண் கையில் இல்லை. அந்த தனியார் மருத்துவமனைக்கு யார் காசு கொடுப்பார்கள்?
இது தான் இன்று வரை இருந்த நடைமுறைச் சிக்கல்.
-oOo-
உதாரணமாக
ஒருவருக்கு விபத்தில் கை எலும்பு முறிந்துள்ளது, இது வரை 108 அம்புலன்ஸ்
அவரிடம் பணம் இருக்கிறதா?, காப்பீடு உள்ளதா?, உறவினர்களால் பணம் செலுத்த முடியுமா? என்ற எந்த கேள்வியும் கேட்காமல்
அவரை அரசு மருத்துவமனைக்குத்தான் அழைத்து செல்லும். அங்கு சென்று அவருக்கு முதலுதவி செய்யப்படும்.
பிறகு உறவினர்கள் எல்லாம் வந்த பிறகு
1. அவர்களிடம் காசு இல்லை என்றால் அவர்கள் அரசு மருத்துவமனையில் சிகிச்சை தொடரலாம்.
2. அவர்களிடம் காசு அல்லது காப்பீடு இருந்தால் வேறு தனியார் மருத்துவமனை செல்லலாம்.
-oOo-
உதாரணமாக,
ஒருவருக்கு விபத்தில் கை எலும்பு முறிந்துள்ளது
அவரிடம் பணம் உள்ளது.
அவர் தனியார் மருத்துவமனை தான் செல்வேன் என்று சொன்னால் அம்புலன்ஸ் அவரை அங்கு அழைத்து செல்வார்கள்.
-oOo-
உதாரணமாக,
ஒருவருக்கு விபத்தில் தலையில் அடிபட்டு மயக்கமாகியுள்ளார். அவர் யார் என்றே தெரியாது. இது வரை 108 அம்புலன்ஸ்
அவரை அரசு மருத்துவமனைக்குத்தான் அழைத்து செல்லும். அங்கு சென்று அவருக்கு முதலுதவி செய்யப்படும்.
பிறகு உறவினர்கள் எல்லாம் வந்த பிறகு
1. அவர்களிடம் காசு இல்லை என்றால் அவர்கள் அரசு மருத்துவமனையில் சிகிச்சை தொடரலாம்.
2. அவர்களிடம் காசு அல்லது காப்பீடு இருந்தால் வேறு தனியார் மருத்துவமனை செல்லலாம்.
-oOo-
இப்பொழுது தமிழக அரசு கொண்டு வந்துள்ள திட்டம் என்ன?
முழுசிகிச்சையில் முதலுதவி பகுதியை மட்டும் தனியாக பிரித்து அந்த முதலுதவிக்கு தமிழக அரசு பணம் கொடுக்கும் என்பது தான்.
இந்த திட்டத்தின் மூலம்
விபத்தில் அடிபட்டவரை அரசு மருத்துவமனைக்குத்தான் கொண்டு வரவேண்டும் என்ற அவசியம் இல்லை.
அருகில் உள்ள தனியார் மருத்துவமனைக்கும் கொண்டு செல்லலாம். முதலுதவிக்கு அரசு பணம் கொடுக்கும் என்பதால்
மருத்துவமனையும் பணம் பற்றி கவலைப்படாமல் சிகிச்சையை துவங்குவார்கள். அவருக்கு முதலுதவி சீக்கிரம் கிடைக்கும்.
பிறகு அவரது உறவினர்கள் வந்த பிறகு அவர்கள் ஆற அமர முடிவு செய்து (இரண்டு நாட்களுக்குள்)
1. காசு அல்லது காப்பீடு இல்லை என்றால் அரசு மருத்துவமனைக்கு வரலாம்
2. காசு அல்லது காப்பீடு உள்ளது என்றால் அதே மருத்துவமனையில் தொடரலாம்
3. காசு அல்லது காப்பீடு உள்ளது என்றால் வேறு தனியார் மருத்துவமனை செல்லலாம்
-oOo-
இதனால் என்ன பலன்?
1. அடிபட்டவருக்கு : உதவி சீக்கிரம் கிடைக்கும். எனவே உயிரை காக்க வாய்ப்பு அதிகம். கை கால் ஆகியவற்றில் அடி பட்டிருந்தால் அந்த உறுப்புகளை காக்கவும் வாய்ப்பு அதிகம்.
2. உறவினர்களுக்கு : ஒருவர் விபத்தில் அடிபட்டார் என்பது அதிர்ச்சி தரும் செய்தி. அந்த நிலையில் அதே மருத்துவமனையில் தொடர்வதா, வேறு எங்கும் செல்வதா, எவ்வளவு காசு ஆகும், கையில் காசு உள்ளதா, கடன் வாங்குவதா, நகையை அடமானம் வைப்பதா என்ற முடிவு எடுக்கவேண்டாம்.
3. தனியார் மருத்துவமனைக்கு: அந்த நபர் அதே மருத்துவமனையில் சிகிச்சையை தொடர்ந்தால், அவர்களுக்கு வருமானம்.
4. அரசிற்கு : மக்களின் உயிரை காக்க முடியும்.
-oOo-
சும்மா இருப்பவர்களை கூட தனியார் மருத்துவமனைகள் பெரிய அடி இருப்பதாக காண்பித்து அதிக கட்டணம் வாங்க முடியுமா ?
முடியாது.
(1) 108 அம்புலன்ஸ்சில் ஒருவர் ஏறும் போதே அவரது உடல்நிலை என்ன என்பது குறித்து அவர்கள் பதிந்துவிடுவார்கள். அதை வைத்தே அவரின் முதலுதவிக்கு எவ்வளவு பணம் தேவை என்பதை சொல்லிவிடலாம்.
(2) விபத்து நடந்த பிறகு காவல் துறையினர் முதல் தகவல் அறிக்கை பதிவார்கள். அதிலும் காயங்களின் தன்மை இருக்கும்.
எனவே இந்த இரண்டையும் வைத்து
இது 100 ரூபாய் முதலுதவியா, (சிராய்ப்பா) 1000 ரூபாய் முதலுதவியா, (கை எலும்பு முறிவா) 10000 ரூபாய் முதலுதவியா, (தொடை எலும்பு முறிவா) அல்லது 1 லட்சம் முதலுதவியா (தலைக்காயம், வயிறு கிழிந்துவிடுவது) என்பதை எளிதில் கண்டு கொள்ளலாம்.
-oOo-
“காவல்துறையும் மருத்துவமனையும் சேர்ந்து ஊழல் செய்வார்கள், எனவே இந்த திட்டத்தை எதிர்க்கிறேன்” என்று கூறுகிறீர்கள் என்றால் avada kedavra என்பதை தவிர சொல்ல எதுவும் இல்லை.
மேலும் அறிந்து கொள்ள இந்த காணொளியை பார்க்கலாம்
மருத்துவம் தொடர்பாக மூத்த எலும்பியல் மருத்துவர் லோகநாதன் சார் அவர்களின் பிற காணொளிகளை இங்கு காணலாம்
IKT – 48 மணி நேரம் நம்மைக்காக்கும் இன்னுயிர் காப்போம் திட்டம்
Creating Emergency Care Fund (IKT Fund)
50 Cr Assurance Mode
Fix ceiling of up to Rs. 1 lakh per individual
Empanelment of Government and Private Hospitals – 609
Integrate the 48 hour cashless scheme with the existing CMCHIS scheme after 48 hours
Selection of 81 Appropriate Packages
IKT Empanelled 609 Hospitals
Government Hospitals
Private Hospitals
Level 1 Hospitals
20
30
50
Level 2 Hospitals
74
157
231
Level 3 Hospitals
121
207
328
215
394
609
The Scope of coverage
If a patient needs admission and minor procedure (listed) which does not exceed 48 hours stay the same may be done at the hospital he/she is being admitted.
If the patient is not stable or requires procedures that may need Hospitalisation beyond 48 hours one of the following conditions may apply.
Stabilization of the patient and Discharge to any empanelled Hospital if the patient needs further treatment which is covered under Chief Minister’s Comprehensive Health Insurance Scheme and is eligible for Coverage.
Stabilization of the patient and Discharge to Government Hospital if the patient needs further treatment but the treatment is not covered under Chief Minister’s Comprehensive Health Insurance Scheme or eligible for Coverage.
Stabilization of the patient and continuation of treatment in same Hospital or any other hospital of his / her choosing if the patient is not willing for transfer to Government Hospital (or) has private Insurance (or) willing to continue treatment as a paid patient.
IKT – Categories of patients who will benefit under NK – 48
All accident victims on road within TN border including tourists from other states and foreigners
Accident victims brought by Good Samaritans
Accident victims brought by family
Accident victims who come by themselves
Unknown accident victim brought by police, or Good Samaritans
Mass casualty accident victims
IKT – NK 48 Exclusion criteria
Assault injuries
Domestic injuries
Fall from height
Injuries due to fall of heavy object
Train traffic accident injuries
Animal bites, Self harm
Occupational work place injuries
Thermal /Chemical/ Burn Injuries
Cracker Blast Injuries
5 Steps of Emergency Trauma Care
Prehospital Triage & Transportation by Ambulance along with in-transit care
Resuscitation & Stabilization in hospital Emergency Department
Damage Control Surgeries
Definitive Care
Rehabilitation
Step 1,2,3 – IKT
Steps 4,5 – KKT – CMCHIS
NK 48 Guideline
On receipt of information from the accident site, Life support ambulance with trained manpower will reach the spot, Triaging & basic resuscitation (cABC) will be done by EMT.
Patients maybe entitled for free treatment upto 48 hours in hospitals of IK – NK 48 Scheme empanelled private hospitals of neighbouring states if the accident occurs within Tamil Nadu but close to the state border.
NK 48 Guideline
5 Levels of triaging at the Accident Scene for guiding the EMT
Pre-hospital Triage & Acuity Scale
Description of the Acuity Scale
Equivalent Triage category
Level 1 – Resuscitation
Patient battling for life in need of resuscitation/Severe hemodynamic compromise/Shock/Traumatic amputation of an extremity
Red
Level 2 – Emergent
Seriously injured patient who requires rapid medical intervention/Penetrating head,chest or abdominal injury/Neurovascular compromise of an extremity
Red
Level 3 – Urgent
Patient with stable vitals, but the presenting problem suggests further evaluation
Minor contusions, abrasions, lacerations not requiring closure, Non urgent with minor complaint
Green
RTA – Patient comes to any Hospital
IK NK 48 Basic Trauma Package for any RTA Patient – Clinical examination ,Hb, Urea, Sugar,ECG,X –Ray Chest. Patient is stable. He will be discharge (Green Category)
Patient in Red / Yellow category
CMCHIS Card Holder(Upto 48 hours) IK – NK48 Empaneled Hospital
Treatment under IK – NK 48 Packages
CMCHIS Non Card Holder / other state / Foreign RTA victims (Upto 48 hours) IK – NK48 Empaneled Hospital
Treatment under IK – NK48 Packages
Packages applicable only Upto 48 Hours in the NK 48 empanelled 609 hospitals only. IFT Can be done within 48 hours based on the triage only among the NK 48 empanelled 609 hospitals
Treatment will be continued under CMCHIS as per existing packages
Non CMCHIS Card holder ( Govt / Pvt empanelled Hospitals under CMCHIS)
Treatment will be continued under free category in Govt Hospitals
Treatment will be continued under payment / pvt insurance by the patient in pvt hospitals
Other state / foreign RTA victims
Treatment will be continued under free category in Govt Hospitals
Treatment will be continued under payment / pvt insurance / PM-JAY by the patient in pvt hospitals
NK 48 Guideline
Critically ill (Red category) patient to be taken by 108 Ambulance service to the nearest empanelled Level 1 Hospital if located within 20-30km.
The Level 1 Hospital may be a Government Hospital or a private facility.
The patient should be transported in the shortest period to ensure advanced trauma life support.
If it is far, the patient should be stabilized in the nearest L2 or L3 hospital and through 108 ambulance should move the patient after stabilization to the L1 facility for definitive intervention.
2 hr mandatory resuscitation for a critically injured patient before any Inter-facility Transfer.
IFT with Pre-Arrival Intimation to the receiving hospital.
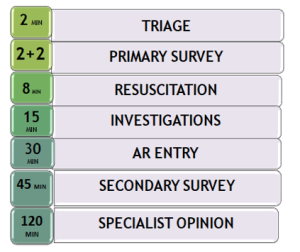
Time Norms in Emergency Care of RTA patients
NK 48 Guideline – Preauth & Claim
EI number should be obtained by the treating hospital, & the URN should be shared even with IFT(Inter facility transfer) Hospital till the treatment course is completed under IKT.
When treatment involves more than 1 hospital, the treatment time will be from the time of admission in the 1st hospital (upto 48 hours only).
NK 48 Guideline – Preauth
Pre-auth submission by Hospital
Within 4 hours of admission during 8 am to 6 pm.
Within 12 hours of admission during 6 pm to 8 am
PREAUTH CRITERIA
Any Identification Card.
If there is no Identity Card, a letter from Hospital to be submitted.
Patient’s Clinical Photo.
Preliminary Assessment Report duly certified by examining Doctor.
AR copy with treating Doctor’s sign.
If the patient needs additional treatment or procedure, Enhancement request may be applied with Secondary Survey report.
CLAIMS CRITERIA
Treatment Summary, Discharge Summary / Referral Letter/ Death Summary within 5 days from the date of admission.
Declaration that no money has been collected from the patient during the course of treatment
CMCHIS URN if available.
All investigations done, with Images.
Operative notes and Case sheet.
Hospital Bills (detailed).
IKT – NK 48 Claims
Claims settlement for NK 48 within 3 days from Claim submission.
CMCHIS call center will make telephonic enquiry on the patient status and keep a record.
Any Death within 1 month of major accident should be reported with PM report for record maintenance.
NK 48 Guideline
Strict follow-up and bench marking of hospitals as per TAEI standards.
Frequent Audits for quality of care
List of Packages
S.NO
Package Name
Rate (in Rs.)
1
TA001 : Central line
4000
2
TA002 : Intraosseous line
4000
3
TA003 : Cervical Collar (philadelphia)
1500
4
TA004 : Endotracheal Intubation
2000
5
TA005 : Tracheostomy
10000
6
TA006 : Oropharngeal Airway
2000
7
TA007 : Blood and Blood Component Transfusion
2000
TA007a : Blood and Blood Component Transfusion – additional uit
பெண்களுக்கு மாரடைப்பு வருவது மிக அரிது. இப்போதைய வாழ்வியல் முறை சகல விதிகளையும் உடைக்கிறது.
மரபியல் ரீதியாக
ஆரோக்யம் குறைவான பெண்கள்
அந்த காலத்தில்
பிறந்த வுடன் கக்குவான் இருமலினாலோ, போலியோவினாலோ
அல்லது காலராவினாமோ
பிரசவத்திலோ இறந்தவிடுவார்கள்
மிகவும் ஆரோக்கியமான மரபணுக்களை உடைய பெண்கள் மட்டுமே 30 வயது தாண்டினார்கள்
எனவே
30 வயதை தாண்டிய பெண் 100 வயது வரை வாழ்ந்தார்
இன்று
மருத்துவம் முன்னேறி விட்டதால்
ஆரோக்யம் குறைவான பெண்கள்
1 வயதில்
11 வயதில்
21 வயதில்
இறப்பது இல்லை
எனவே
அவர்களுக்கு மாரடைப்பு வருகிறது
இன்று 50 – 60 வயதில் மாரடைப்பு வந்து இறக்கும் பெண்கள் எல்லாம்
1980களுக்கு முன்னர்
50 வயது வரை வாழ்ந்திருக்கவே மாட்டார்க்ள்
பிரசவத்திலேயே
அல்லது
அதற்கு முன்னரோ இற்ந்திருப்பார்கள்
மாரடைப்பு வரும் மரபணுக்கள் உள்ள பெண்கள்
மாரடைப்பு வரும் வயது வரை வாழ்ந்து
பெண்களுக்கு மாரடைப்பு வருவது மிக அரிது.
இப்போதைய வாழ்வியல் முறை சகல விதிகளையும் உடைக்கிறது
அவர்களை அந்த வயது வரை வாழ வைக்கிறது
1. If a new consultant shows up ,showers “abuses”(literal) in OT,just because out of 90 patients, 89 RTPCR were sent in 2 hours timeline and one was missed.( One of the many examples)
2. Always shows that the students are absolutely poor in everything.
Yes,she/he teaches .
Asked by people around to accept the tantrums and abuses ,because the teacher is good.
But,
How long will this culture and attitude continue ?
Isn’t it a high time to stop passing down the same tantrums , which you were part of in your residency (in the other top institute of country and a good name worldwide) ?
I don’t agree with this, that – We learn under stress/upon listening “kind” words.
Opinions/ Suggestions please.
My Answer
There can Three possibilities
1
The consultant behave the same with every one – staff, OT Technician etc
2
The consultant behaves like this only with students, but nice with other cadres
3
The consultant behave the nice with all others (including other students) but is nasty only with you
-oOo-
1
If the consultant behave the same with every one –> then it is his nature. It requires a long term correction. Being a resident, it is not your job. Just follow the EIEO Policy (ear in ear out – means, don’t take words beyond your auditory nerve into your cortex)
2
If the consultant behaves like this only with students, but nice with other cadres, then it is a result of the misconception that “Abusers are best teachers and abused students are best students” . . . Sadly, there are many doctors who support this even today . . . You can’t do much except taking a pledge that you won’t abuse your students when you become a teacher
3.
If the consultant behave the nice with all others (including other students) but is nasty only with you, the fault may be with you or with him/her
If the fault is with you, correct yourself
If the fault is with him/her, change the Unit





 2000களின் ஆரம்பம் முதல் இன்று வரை மிக அதிகமாக தேவைப்படும் ஒரு திறமை (பழைய படங்களை புதுப்பிற்பது) இனி பின்னால் சென்று விடும்
2000களின் ஆரம்பம் முதல் இன்று வரை மிக அதிகமாக தேவைப்படும் ஒரு திறமை (பழைய படங்களை புதுப்பிற்பது) இனி பின்னால் சென்று விடும் முதலுதவிக்கு 1 லட்சமா என்று கேள்வி எழுகிறதா ?
முதலுதவிக்கு 1 லட்சமா என்று கேள்வி எழுகிறதா ? முதல் வகை + இரண்டாம் வகை இரண்டுமே ஸ்பாட் அவுட் தான்
முதல் வகை + இரண்டாம் வகை இரண்டுமே ஸ்பாட் அவுட் தான் இதனால் என்ன பலன்?
இதனால் என்ன பலன்?



 There can Three possibilities
There can Three possibilities