நீண்ட பதிவு : பொறுமையாக வாசிக்கவும்
1
இரத்தக்குழாய்களில், தமனிகளில் ஏற்படும் வீக்கத்திற்கு தமனிக்கொப்புளம் என்று பெயர். இதை ஆங்கிலத்தில் அனிருசம் aneurysms என்று அழைப்பார்கள். மூளைக்குள் இருக்கும் தமனிகளில் சில நேரங்களில் இது போன்ற வீக்கங்கள் ஏற்படுவதுண்டு. இதை விட்டு விட்டால் எந்நேரம் வேண்டுமானாலும் இது வெடித்து அதனால் மூளைக்கும் இரத்தக்கசிவு ஏற்படலாம். சிறிதளவு மட்டுமே இரத்தம் கசிந்தால் சிகிச்சை அளித்து அந்த நபரை காப்பாற்ற முடியும். அதிக அளவு இரத்தம் கசிந்தால் அது உயிருக்கு ஆபத்தாக முடியும்
எனவே இது போன்ற வீக்கம் இருப்ப்தை கண்டு பிடித்தவுடன் அறுவை சிகிச்சை செய்து கிளிப் ஒன்றை அங்கு பொறுத்தி வீக்கம் வெடிக்காமல் செய்யவேண்டும். சில நேரங்களில் மூளையின் உள்ளே, எளிதில் அறுவை சிகிச்சை செய்ய முடியாத இடங்களில் வீக்கங்கள் இருந்தால் குருதி குழாய் வழியாகவே சுருள்கள் (coil) மற்றும் குருதி வழி திருப்பி (flow diverter) ஆகியவை மூலம் சிகிச்சை அளிக்கலாம்.
இவை அனைத்தும் மிகவும் நுணுக்கமான, நவீன கருவிகள் மற்றும் மிகுந்த திறன் தேவைப்படும் சிகிச்சை முறைகள்
பொதுவாகவே மூளையில் செய்யப்படும் அறுவை சிகிச்சை தேவைப்படும் படிப்பு, பயிற்சி, திறமை ஆகியவை அடிகம். அதனால் தான் அறுவை சிகிச்சை செய்யப்படும் பல மருத்துமனைகளில் மூளை அறுவை சிகிச்சை செய்யப்படுவதில்லை
இது போன்ற அறுவை சிகிச்சைகளை செய்ய
1. அறுவை அரங்கில் நுண்ணோக்கி (Operating Microscope)
2. நுண் அறுவை சிகிச்சை செய்யும் கருவிகள் (Micro surgery instruments)
3. மூளை அறுவை சிகிச்சை நிபுணர் (Neurosurgeon)
4. மயக்கவியல் நிபுணர் (Anaesthesiologist)
5. அறுவை அரங்க செவிலியர் (Theatre Nurse)
6. அறுவை அரங்க நுட்பனர் (OT Technician)
தேவை என்பதால் மூளை அறுவை சிகிச்சை செய்யப்படும் பல மருத்துவமனைகளில் கூட தமனிக்கொப்புளத்திற்கான அறுவை சிகிச்சைகள் செய்யப்படுவதில்லை.
பல நாடுகளில் இந்த அறுவை சிகிச்சை செய்யப்படுவதில்லை. இந்தியாவிலும் கூட சில மாநிலங்களில் செய்யப்படாததால் தான் நோயாளிகள் சென்னை வருகிறார்கள்
2
விழுப்புரம் அரசு மருத்துவக்கல்லூரி 2010ஆம் ஆண்டில் ஆரம்பிக்கப்பட்டது. தமிழகத்தில் இருக்கும் பல மருத்துவக்கல்லூரிகளை விட அது புதிது தான்.
3
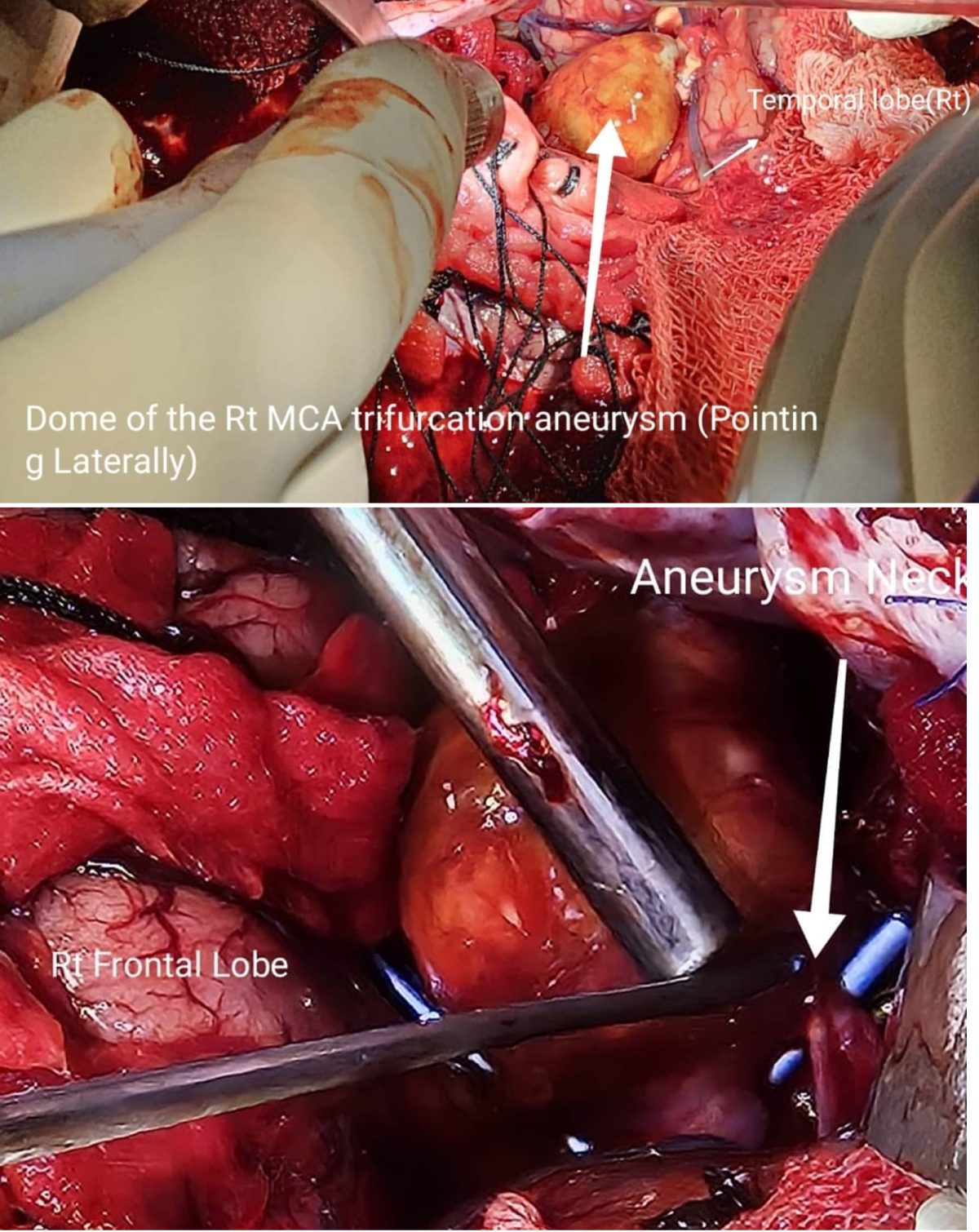
மூளையில் உள்ள பெருமூளை நடுத்தமனியில் (MCA Middle Cerebral Artery) ஏற்பட்ட சிக்கலான முக்கூறு (Trifurcation) தமனிக்கொப்புளத்தால் (Aneurysm) பாதிக்கப்பட்ட நோயாளி ஒருவருக்கு விழுப்புரம் அரசு மருத்துவமனையிலேயே அறுவை சிகிச்சை செய்யப்பட்டுள்ளது. மூளை முதுகுத்தண்டு நரம்பியல் அறுவை சிகிச்சை நிபுணர்கள் மரு.பல்லவன், மரு.சந்தோஷ், மரு. ராஜ்கவுதம் ஆகியோருக்கு பாராட்டுக்கள்
தமிழக அரசு மருத்துவத்துறையில் இருக்கும் நவீன கருவிகள், மற்றும் மருத்துவர்களில் திறமை, அர்ப்பணிப்பு ஆகியவற்றில் ஆழத்தையும் அகலத்தையும் இது பறைசாற்றுகிறது
-oOo-
இதே போல் மூளையின் உட்கழுத்துத் தமனியில் (Internal Carotid Artery) ஏற்பட்ட தமனிகொப்புளத்திற்கு (aneurysm) சில நாட்கள் முன்னர் பிரபல தமிழ் திரைப்பட நடிகர் சென்னையின் தனியார் மருத்துவமனையில் சிகிச்சை பெற்றார். அதே பிரச்சனைக்கு, தனது வீட்டின் அருகிலேயே, முற்றிலும் இலவசமாக ஒருவருக்கு அறுவை சிகிச்சை செய்யப்பட்டுள்ளது.
189 வயதான மெட்ராஸ் மருத்துவக்கல்லூரியிலோ, அல்லது மதுரை, கோவை போல் தமிழகத்தின் ஓரிரண்டு இடங்களில் மட்டும் இது நடக்கவில்லை
தமிழகத்தில் 25க்கு மேற்பட்ட இடங்களில் இது போன்ற நவீன உயர்தர அறுவை சிகிச்சைகள் தினந்தோறும் நடந்து கொண்டு தான் உள்ளன
பல நாடுகளில் இந்த அறுவை சிகிச்சையை செய்யும் வசதி இல்லை
சில நாடுகளில் ஓரிரண்டு நிலையங்களில் மட்டுமே இதை செய்ய முடியும்
அதுவும் அமெரிக்கவில் இதற்கு கட்டணம் $138,000
தனது வீட்டில் இருந்து 50 கிலோமீட்டருக்குள் இருக்கும் ஒரு மருத்துவமனையின் மூளையில் ஏற்பட்ட தமனிக்கொப்புளத்திற்கு அறுவை சிகிச்சை செய்து கொள்ளவும் வசதி உள்ளதும் அதுவும் இலவசமாக செய்து கொள்ளலாம் என்பதும் தான் தமிழக மருத்துவத்துறையின் சிறப்பு
சில நாடுகளில் இந்த அறுவை சிகிச்சைக்கும் காலம் மிகவும் அதிகம் எனப்தால் தமனிக்கொப்புளம் வெடித்து விடுகிறது
-oOo-
மூளையில் இருக்கும் இரத்தக்குழாய்களில் வெடிப்பு ஏற்பட்டால் என்ன ஆகும் ?
வெடிப்பு ஏற்பட்ட இரத்தக்குழாய் என்ன வகையானது, அது எங்குள்ளது என்பதை பொறுத்து பல பிரச்சனைகள் வரலாம்
மூளைக்குள் இருக்கும் இரத்த குழாய்களில் வெடிப்பு ஏற்பட்டால் மூளைக்கு இரத்த கசிவு ஏற்படலாம் (Intra cerebral Hemorrhage)
அதே நேரம் மூளைக்கு செல்லும் தமணிகளில் வெடிப்பு ஏற்பட்டால் இரத்த கசிவு மூளையின் மேல் உள்ள மெல்லிய உரை (arachnoid membrane) மற்றும் மூளைக்கு இடையில் (sub arachnoid bleed) ஏற்படலாம்
இது போல் மூளைக்கும், மூளைக்கு வெளியில் இருக்கும் மெல்லிய உரையான அராக்னாய்ட் சவ்விற்கும் இடையில் ஏற்படும் இரத்த கசிவை Sub Arachnoid Hemorrhage என்று அழைக்கிறார்கள்
அப்படி ஏற்படும் போது
1. அந்த இரத்த கசிவு தொடர்ந்து கொண்டிருந்தால் நபர் இறந்து விடுவார்
2. (தானாக உறைந்து) இரத்த கசிவு நின்றால் கூட இரு வித பாதிப்புகள் ஏற்படலாம்
முதலாவதாக
இந்த மூளைக்கு வெளியில் இருக்கும் மெல்லிய உரையான அராக்னாய்ட் சவ்விற்கும் இடையில் உள்ள இடத்தில் (sub arachnoid space) மூளை தண்டுவட நீர் (CSF, Cerebro Spinal Fluid) இருக்கும். அதன் வழியாகத்தான் பிற இரத்தக்குழாய்கள் செல்லும். இந்த இடத்தில் இரத்தம் வந்தது என்றால் பிற இரத்தக்குழாய்கள் சுருங்கி (vasospasm) அதனால் மூளைக்கு செல்லும் இரத்த ஓட்டம் பாதிக்கப்பட்டு மூளையின் திசுக்கள் வேலை செய்யாமல் (ischemia) போகலாம். அல்லது இறந்து (infarct) போகலாம்
3
இரண்டாவதாக மூளை தண்டுவட நீரில் (CSF, Cerebro Spinal Fluid) இரத்தம் கலப்பதால் அந்த நீர் செல்லும் பாதையில் அடைப்பு ஏற்பட்டு, அந்த நீர் வெளியில் செல்லாமல், மூளைக்குள் அதிக அழுத்தம் ஏற்படலாம்
எனவே
ஒருவருக்கு மூளையின் மேல் உள்ள மெல்லிய உரை (arachnoid membrane) மற்றும் மூளைக்கு இடையில் இரத்தக்கசிவு ஏற்பட்டால் (sub arachnoid bleed) நாம் செய்யவேண்டிய விஷயங்கள் மூன்று
1.
எதனால் இரத்தக்கசிவு ஏற்பட்டுள்ளது என்பதை கண்டறிந்து அதை நிறுத்த முயலவேண்டும். மீண்டும் இரத்த கசிவு ஏற்படாமல் தடுக்க வேண்டும்
2.
இரத்தக்குழாய்கள் சுருங்கியிருந்தால் அதை விரிய வைக்க வேண்டும்
3.
மூளைக்குள் நீர் செல்லும் பாதையில் அடைப்பு ஏற்பட்டிருந்தால் நீர் வெளியேற மாற்றுப்பாதை கண்டு பிடிக்க வேண்டும்
-oOo-
1
எதனால் இரத்தக்கசிவு ஏற்பட்டுள்ளது என்பதை கண்டறிய உள்ளுறுப்பு ஊடு பதிவி இரத்தநாளச் நிழல் படம் (சிடி ஆஞ்சியோ) அல்லது எண்ணிம இரத்தநாள நிழல் படம் (digital subtraction angiogram) செய்ய வேண்டும்
2
இரத்தக்குழாய்கள் சுருங்கியிருந்தால் அதை விரிய வைக்க மருந்து கொடுக்கவேண்டும்
3
மூளைக்குள் நீர் செல்லும் பாதையில் அடைப்பு ஏற்பட்டிருந்தால் நீர் வெளியேற அறுவை சிகிச்சை மூலம் மாற்றுப்பாதை ஏற்படுத்த வேண்டும்
4.
எதனால் இரத்தக்கசிவு ஏற்பட்டுள்ளது என்பதை கண்டறிந்த பிறகு அந்த பிரச்சனைக்கு அறுவை சிகிச்சை மூலமோ ஆஞ்சியோ மூலமோ வைத்தியம் செய்யவேண்டும்
-oOo –
மூளைக்குள் இரத்தக்குழாய் வெடிக்கும் போது அது பெரிய வெடிப்பு என்றால் அந்த நபர் இறந்து விடுவார்
சிறு வெடிப்பு என்றால் தலைவலி வரும்
-oOo –
நடைமுறையில் என்ன நடக்கிறது என்றால்
தலைவலியுடன் மருத்துவமனை செல்பவருக்கு ஸ்கேன் செய்து பார்த்து விட்டு இரத்த கசிவு என்று சொல்வார்கள்
எங்கு என்று சொல்லமாட்டார்கள். ஏனென்றால் அவர்களுக்கே தெரியாது
அடுத்து இரத்தக்குழாய்கள் சுருங்கியிருந்தால் அதை விரிய வைக்க மருந்து கொடுக்கவேண்டும் என்பதால் தீவிர பிரிவில் வைத்திருப்பார்கள்.
ஒரு வேளை அழுத்தம் அதிகரித்தால் அதற்கு அறுவை சிகிச்சை செய்யவேண்டும் என்பார்கள். இந்த அறுவை சிகிச்சையினால் இரத்த கசிவு நிற்காது என்று மருத்துவர்கள் கூறுவார்கள். இரத்த கசிவை நிறுத்தாமல் ஏன் அறுவை சிகிச்சை என்று நோயாளியின் உறவினர்கள் குழம்புவார்கள்
இந்த குழப்பங்களுக்கு காரணம் என்னவென்றால் இந்த பிரச்சனையின் தன்மை அப்படி. நோய் என்ன, எதனால், பாதிப்பு எவ்வளவு என்று முதல் இரு தினங்கள் யாராலும் கூற முடியாது. அனைத்து பரிசோதனைகளையும் செய்த பிறகு தான் தெளிவு வரும்.
அதற்குள் மூன்று நான்கு மருத்துவமனை மாற்றினால் சிக்கல்கள் அதிகரிக்கவே செய்யும்

 There can Three possibilities
There can Three possibilities