James Marion Sims (January 25, 1813 – November 13, 1883) was an American physician and a pioneer in the field of surgery, known as the “father of modern gynaecology”.His most significant work was the development of a surgical technique for the repair of vesicovaginal fistula, a severe complication of obstructed childbirth. He is also remembered for inventing Sims’ speculum, Sims’ sigmoid catheter, the Sims’ position, use of silver wire as a suture, Insemination and postcoital test, and argued for the admission of cancer patients to the Woman’s Hospital, despite contemporary beliefs that the disease was contagious.
He also advocated a laparotomy to stop bleeding from bullet wounds to this area, repair the damage and drain the wound. His opinion was sought when President James Garfield was shot in an assassination attempt; Sims responded from Paris by telegram. Sims’ recommendations later gained acceptance.
In 1878, Sims drained a distended gallbladder and removed its stones. He published the case believing it was the first of its kind; however, a similar case had already been reported in Indianapolis in 1867
But, Of Late, There are many people who try to intentionally portray him in negative light
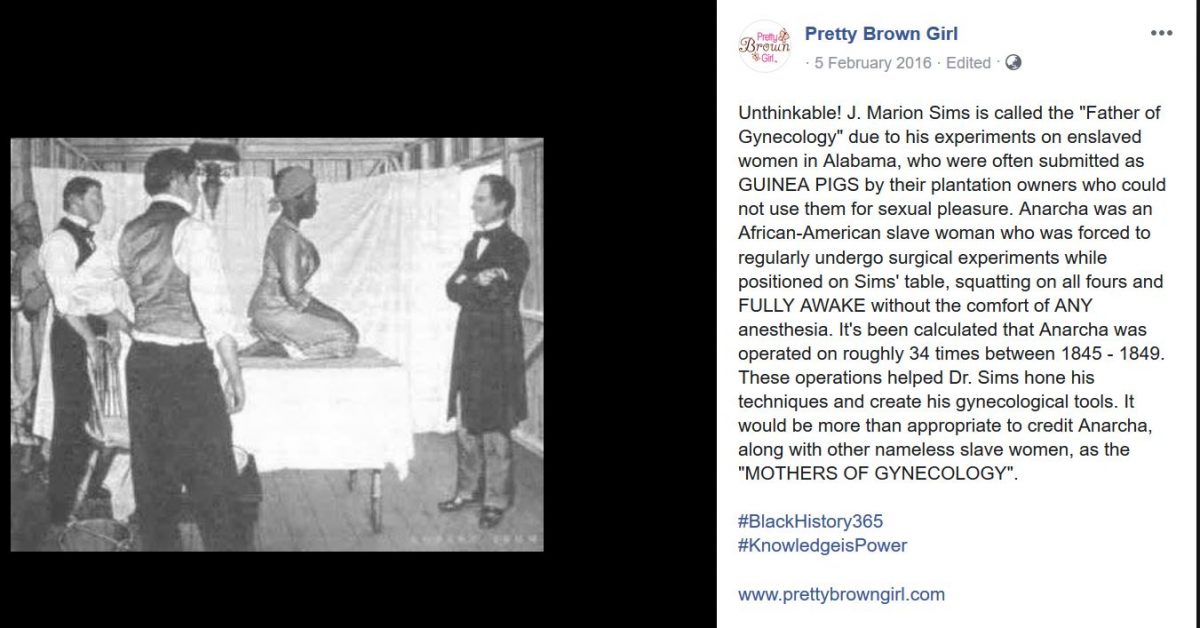
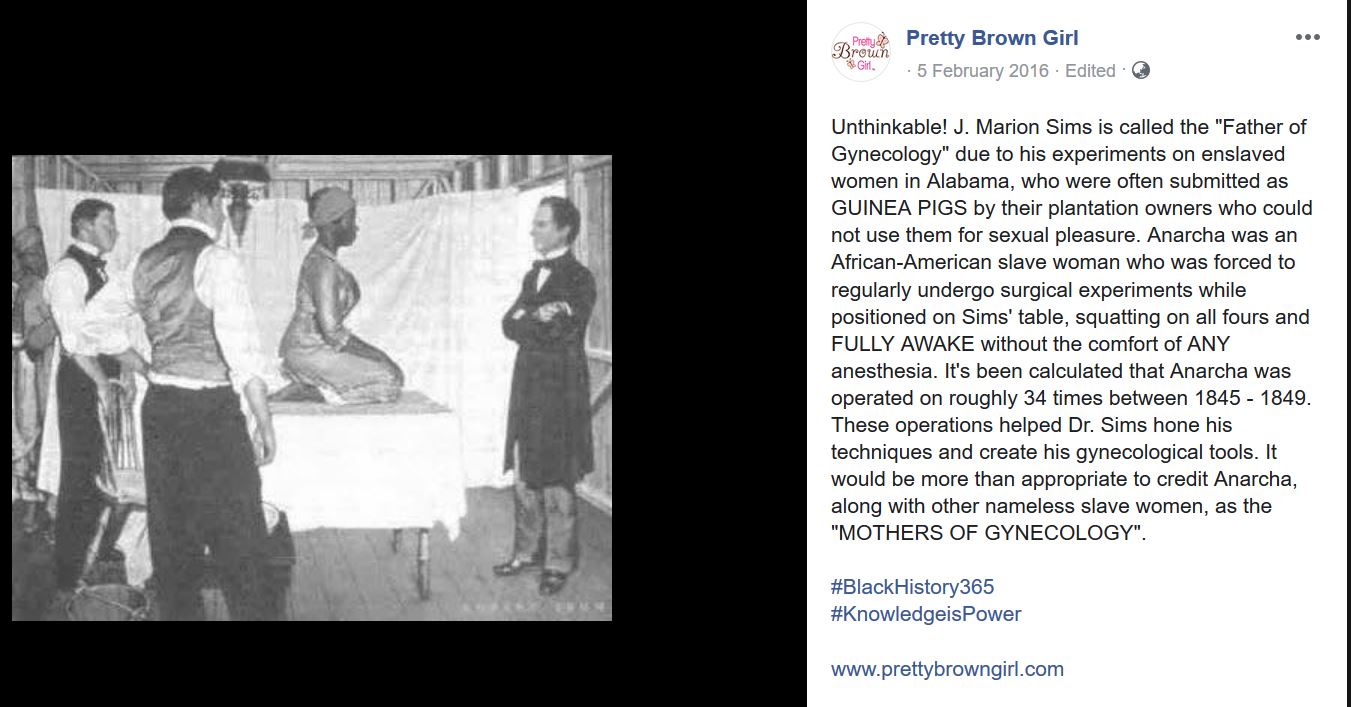
Here is one such Facebook post https://www.facebook.com/prettybrowngirls/photos/a.190238547702360/1035669863159220/?type=3
Unthinkable! J. Marion Sims is called the “Father of Gynecology” due to his experiments on enslaved women in Alabama, who were often submitted as GUINEA PIGS by their plantation owners who could not use them for sexual pleasure. Anarcha was an African-American slave woman who was forced to regularly undergo surgical experiments while positioned on Sims’ table, squatting on all fours and FULLY AWAKE without the comfort of ANY anesthesia. It’s been calculated that Anarcha was operated on roughly 34 times between 1845 – 1849. These operations helped Dr. Sims hone his techniques and create his gynecological tools. It would be more than appropriate to credit Anarcha, along with other nameless slave women, as the “MOTHERS OF GYNECOLOGY”.
On Reading it, You will immediately Hate the Man because of the following issues
- //his experiments on enslaved women //
- //submitted as GUINEA PIGS //
- //plantation owners who could not use them for sexual pleasure. //
- //positioned on Sims’ table, squatting on all fours //
- //FULLY AWAKE //
- //comfort of ANY anesthesia. //
- //roughly 34 times between 1845 – 1849. //
- //hone his techniques and create his gynecological tools.//
So
The impression Any Lay Person as well as Few Doctors with low IQ Gets with this Writeup is that
Dr Sims Made Experiments on a slave, and was cruel that he made it when she was awake and the only reason the slave had to undergo the surgery is for the sexual pleasure of the slave’s owner
But, When we examinite it more carefully it is easy to conclude that it is a rubbish Writeup, itt is biased and written with a perverted intention to make some one hate SIMS
Let us examine the points one by one
//his experiments on enslaved women //
//submitted as GUINEA PIGS //
Guinea Pigs are used in Experimentation for various purposes
The Pigs are usually normal and are sacrificed for sake of trial
If the procedure is not done, the Guinea Pig does not have any problem
But
Clinical Trial is Different
Here the person already has a disease
and undergoes the procedure
WHICH CAN CURE HIM/HER
or
MAIM / KILL HIM / HER
Use of Guinea Pig and Experiments in this write up is malafide
//plantation owners who could not use them for sexual pleasure. //
As if the only indication for VVF is sexual Pleasure
And the woman is otherwise very happy with VVF and RVF?
What is Vesico Vaginal Fistula – It is a condition in which Urine will come via Vagina continously and without any control. What is Recto Vaginal Fistula – It is a condition in which Feces (Stool or Shit) will come via Vagina continously and without any control. Do you think a woman with such condition will like it. Do you think that she will have to be forced to undergo the surgery. Not at all. Women with such conditions were running from pillar to post to get cure. And there was NO CURE Available at the time, and one doctor offered to cure them, but said he also did not have any experience. So What should have been done ? To try the procedure or just to leave the women with urine and feces dribbling continously through their vagina ?
//positioned on Sims’ table, squatting on all fours //
You can also describe Lithotomy and give an grotesque impression to the lay public
//FULLY AWAKE //
//comfort of ANY anesthesia. //
These two lines actually take the cake
These will create immense anger and make blood boil
Isn’t it
But Wait
When were these done
//roughly 34 times between 1845 – 1849. //
Oh
So the surgeries were done before October 16, 1846 and also just two years after October 16, 1846
What is 16/10/1846 by the way
Find it yourself
Then you will understand the height of perversion the author had gone by using the words “FULLY AWAKE” and “comfort of ANY anesthesia”
//hone his techniques and create his gynecological tools.//
This is the only correct line in the writeup
-oOo-
This is how, You can fool an unsuspected reader Hate some one by making normal actions look like Big Crime
By the way
Did you find the significance of 16/10/1846 at least now
Well that was when Ether was FIRST used
So
What does this writeup do
It blames Sims of not using Anaesthesia for an surgery done before Anaesthesia was invented
This is why I call this writeup as peak of perversion and summit of lies
For the Serious Readers, there is a detailed writeup in Journal of Medical Ethics. You can also read it J Med Ethics. 2006 Jun; 32(6): 346–350. doi: 10.1136/jme.2005.012559 PMCID: PMC2563360 PMID: 16731734
I did not see the article when I wrote this post
 The pharmacist, who had to PREPARE THE DRUG, had to be very careful. Adding 5gm of a substance when 5 mg has to be added would be fatal. Hence Pharmacy was a specialist discipline and A Pharmacist was needed for each and every medical shop. That was the time such regulations were made. Only in that backdrop, it was made that a Pharmacy needs a Pharmacist
The pharmacist, who had to PREPARE THE DRUG, had to be very careful. Adding 5gm of a substance when 5 mg has to be added would be fatal. Hence Pharmacy was a specialist discipline and A Pharmacist was needed for each and every medical shop. That was the time such regulations were made. Only in that backdrop, it was made that a Pharmacy needs a Pharmacist Medicine has been evolving. Disciplines like Grief counselling, Nutrition, Diet, Transplant Co ordinator etc are coming up
Medicine has been evolving. Disciplines like Grief counselling, Nutrition, Diet, Transplant Co ordinator etc are coming up That is really appreciable. But at the same time, we need to also educate the police and in case the patient requires surgery, it is better to keep the stomach free of any fluids. Of course, accident victims will feel thirst due to two mechanism (1) Blood Loss –> Hypovolemia (2) Sympathetic System Surge –> Dry Mouth , but don’t give anything by mouth till treatment plan is finalised
That is really appreciable. But at the same time, we need to also educate the police and in case the patient requires surgery, it is better to keep the stomach free of any fluids. Of course, accident victims will feel thirst due to two mechanism (1) Blood Loss –> Hypovolemia (2) Sympathetic System Surge –> Dry Mouth , but don’t give anything by mouth till treatment plan is finalised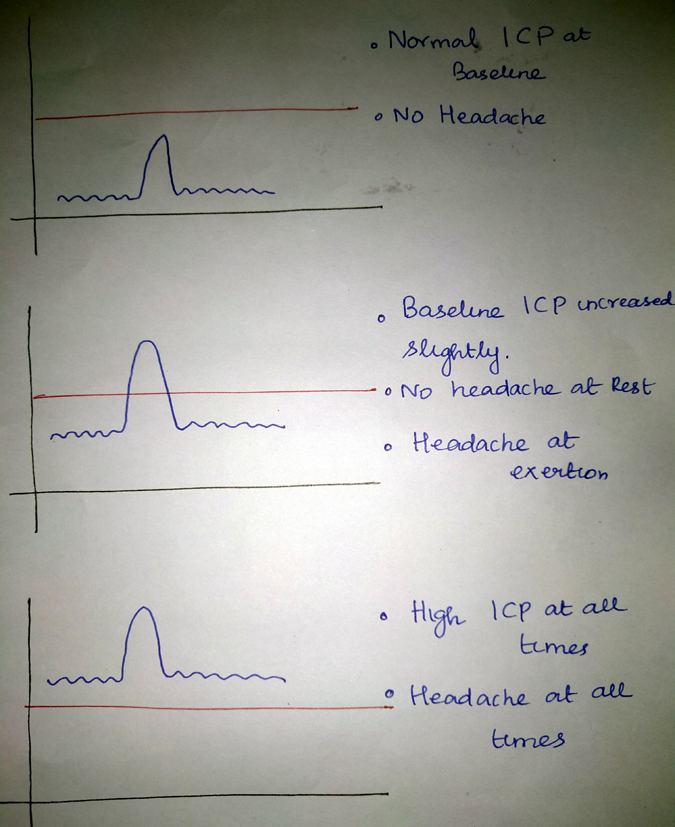

 I did an Clinical Examination and as expected the Fundus (Eye) showed early eigns of increased pressure inside the skull. It can be any infection or tumour. MRI of Brain Revealed Infection of the coverings of the brain with Tuberculous bacteria. The patient took proper treatment and the infection has been cured and the pressure has come back to normal and when you see the Eye (Fundus) now, there is no sign of raised pressure
I did an Clinical Examination and as expected the Fundus (Eye) showed early eigns of increased pressure inside the skull. It can be any infection or tumour. MRI of Brain Revealed Infection of the coverings of the brain with Tuberculous bacteria. The patient took proper treatment and the infection has been cured and the pressure has come back to normal and when you see the Eye (Fundus) now, there is no sign of raised pressure
 Shopping means getting possession of a new article
Shopping means getting possession of a new article