அமேசன் கிண்டில் போட்டி 2019ல் முதல் பரிசு பெற்ற கதை
இடம் : முதலிடம்
-oOo-
போட்டியின் கடைசி நாளன்று புத்தகம் வெளியிட்டு இரண்டே வாரங்களில் புருனோ எப்படி முதல் கட்டத்தில் வென்று அடுத்த கட்டம் சென்றார் என்று பலரும் கேட்கிறார்கள் ? என்னிடம் யாரும் நேரடியாக கேட்கவில்லை என்பதால் இது குறித்து பதில் கூறவேண்டாம் என்று நினைத்தேன். ஆனால் ரவியும், சென்னும் அனைவரையும் ஒன்று போல் நடத்தவில்லை என்றும் சிலரது புத்தகங்களுக்கு மட்டும் உதவினார்கள் என்று அவர்கள் மேல் குற்றச்சாட்டு வந்ததால் சில விஷயங்களை பொதுவில் கூறலாம் என்று நினைக்கிறேன். எனவே சிறு வரலாறு
பி.எஸ்.என்.எல் இணைய இனைப்புடன் இலவசமான வந்த சிறு இணைய இடத்தில் தான் (வெப் ஹோஸ்டிங் ஸ்பேஸ்) நான் முதலில் எனது வலைத்தளத்தை நடத்தினேன். அந்த காலத்தில் எனக்கு எச்.டி.எம்.எல் தெரியும். அதன் மூலம் தளத்தை கட்டமைத்தேன். அத்துடன் யாகூ வழங்கிய ஜியோசிட்டீசிலும் சில கோப்புகள் இருந்தன.
ஒருமுறை அகில இந்திய பட்டமேற்படிப்பு நுழைவுத்தேர்வு முடிந்தவுடன் அந்த கேள்விகளுக்கான விடையை விரிவாக என் தளத்தில் எழுதினேன். அதாவது என்ன விடை, இது எந்த நூலில் உள்ளது, இது குறித்து அடிப்படை விபரங்கள் என்ன, இந்த ஒரு விடை சரி என்றால் ஏன் மீதி மூன்று விடைகளும் தவறு. மேலும் அறிந்து கொள்ள வேண்டிய விஷயங்கள் உள்ளனவா, இந்த கேள்வி எதாவது ஒரு நூலில் மட்டும் உள்ளதா, எளிதாக ஞாபகம் வைத்துக்கொள்ள உத்திகள் (நிமோனிக்ஸ்) என்ன என்று விரிவாக என் தளத்தில் எழுத ஆரம்பித்தேன்
அதுவரை நுழைவுத்தேர்வு நூல்களில் கேள்வி மற்றும் அதற்கான விடை ஏ,பி,சி,டி இருக்கும். அது எந்த நூலில் உள்ளது போன்ற விபரங்கள் இருக்காது. எனவே நான் எழுதிய பாணி வெற்றி பெற்றது. அது என்ன பாணி என்று அறிய மறுமொழிகளில் சுட்டி 1 பார்க்கவும். வரவேற்பு அதிகரிக்கவே TargetPG (மறுமொழிகளில் சுட்டி 2) என்ற வலைத்தளத்தை வாங்கி, அதில் வோர்ட்பிரசை நிறுவி தளம் நடத்தினேன்.
அந்த நேரம் கூகிளும் ப்ளாக்கர் என்ற சேவையை வழங்கியது. வோர்ட்பிரஸ் அனுபவம் இருந்தால், கூகிளில் doctorbruno.blogspot.com என்று ஒரு கணக்கு துவங்கி அதில் என் வலையுலக பயணம் துவங்கியது. மருத்துவ பட்டமேற்படிப்பு குறித்த விபரங்கள் TargetPG comமிலும், பிற விபரங்கள் doctorbruno.blogspot.comமிலும் வந்து கொண்டிருந்தன
TargetPG com தளத்தில் ஒரு பக்கத்தை ஏற்றிபிறகு, அது குறித்து யாராவது தேடினால் என் தளத்தின் பக்கம் கூகிளில் வர சில நாட்கள் ஆனது. அதே நேரம் doctorbruno.blogspot.comமில் நான் எழுதுவும் விஷயம் சில மணிநேரங்களிலேயே கூகிளில் வந்தது. ஏனென்றால் BLOGSPOTல் இருக்கும் தளங்களை கூகிள் முதலில் இண்டெக்ஸ் செய்து யாராவது தேடினால் உடனே நம் தளம் தேடலுக்கான விடைகளில் வந்தது என்பதை இரு தளங்களின் StatCounter புள்ளிவிபரங்கள் கற்றுத்தந்தன. எனவே TargetPG net என்ற தளத்தை துவங்கி ப்ளாக்கரின் எப்.டி.பி மூலம் நமது வழங்கியில் வலைத்தளத்தை பதிப்பிக்கும் சேவை மூலம் உடனுக்குடன் செய்திகள் போட பயன்படுத்தினேன். பிறகு DNS சேவை வந்தபிறகு, இந்த தளம் கூகிளில் வழங்கிகளிலேயே இருந்தது. பிறகு www mcqsonline com www pgmed org www medicalbooks in போன்று பல தளங்கள் சேர்ந்தன.
AIIMS, PGI Chandigarh, JIPMER, தமிழ்நாடு அரசு மருத்துவ பட்டமேற்படிப்பு நுழைவுத்தேர்வு போன்ற தேர்வுகளின் முடிவு வந்த உடன், அந்த கோப்பை என் தளத்தில் ஏற்றுவது வழக்கம். அப்பொழுது எல்லாம் தரவு நிலையங்கள் (டேட்டாசெண்டர்) அவ்வளவு பிரபலமாகாத நேரம். மருத்துவ பட்டமேற்படிப்பு தேர்வுகள் நடத்துபவர்கள் (கல்லூரிகள், பல்கலைகழகங்கள், தேர்வு குழுக்கள்) எல்லாம் அவர்கள் அலுவலகத்தில் இருக்கும் வழங்கியையே பயன்படுத்துவார்கள். தேர்வு சமயத்தில் ஒரே நேரத்தில் பல ஆயிரம் பேர் தொடர்பு கொள்வதால் வழங்கி எல்லாம் தொங்கிவிடும். ஆனால் www targetpg net கூகிள் வழங்கியில் இருந்ததால் தொங்காது எனவே முடிவு வரும் நாளன்று கண்கொத்தி பாம்பு போல் காத்திருந்து முடிவு வந்த உடன், அந்த கோப்பை தரவிரக்கி, என் தளத்தில் ஏற்றி விடுவேன். பலமுறை முடிவு வெளியான தளம் “தொடர்பு எல்லைக்கு அப்பாற்பட்டு” இருக்கும் போது www targetpg netல் மட்டும் முடிவுகள் தெரியும்.
(பிற்காலத்தில் தமிழக அரசின் உறுப்பு மாற்று அறுசை சிகிச்சை தொடர்பான முக்கியமான தரவு தளத்தை நடத்தும் பொறுப்பு என்னிடம் வந்தது. பல வருடங்கள் நான் நடத்தினேன். யாராலும் கொந்த (ஹேக் செய்ய) முடியவில்லை. யானை வித்தை குதிரை வித்தை எதுவும் பலிக்கவில்லை. தரவு தளம் இருந்தது கூகிள் டிரைவில். கூகிள் இது போல் பல வசதிகளை தந்தது, தருகிறது. ஆனால் பலரும் அதை பயன்படுத்துவது இல்லை.)
இப்படியாக www targetpg net பிரபலமானது. பிறகு www.targetpg.comம் www.targetpg.netம் சேர்ந்து www targetpg in (மறுமொழிகளில் சுட்டி 3) ஆனது. ஆரம்ப கட்டத்தில் அது புளோரசண்ட் பச்சை, பிங்க், மஞ்சள் என்றெல்லாம் இருந்தது. 2010க்கு பிறகு தனசேகர் நிறத்தை மாற்ற சொன்னதான் தளத்திற்கு கொஞ்சம் டீசண்ட் லூக் வந்ததும், 2013ல் ரவி தளத்தை வேகமாக மாற்றித்தந்ததும் வரலாறு.
நான் சன்சார்நெட் தளத்தில் கேள்விகளுக்கான பதிலை எழுத துவங்கிய காலத்தில் ஒரு முறை ஒருவர் அலைபேசினார். (தளத்தில் என் அலைபேசி எண் இருந்தது) நான் விடைகளை எழுதும் முறை நன்றாக இருக்கிறது என்றும் அந்த வருட வினாத்தாளில் இருக்கும் 300 கேள்விக்களுக்கும் அது போல் எழுதி தர முடியுமா என்றும் கேட்டார். சரி என்று சொன்னேன். உடனே குறுஞ்செய்தியில் என் முகவரி கேட்டார், அனுப்பினேன். நன்றி JP Vij என்று பதில் வந்தது. அதை விட்டு விட்டேன்.
இரண்டு நாட்கள் கழித்து கூரியர் ஒன்று டெல்லி Jaypee Publishersல் இருந்து வந்தது. பிரித்து பார்த்தால் அகில இந்திய நுழைவுத்தேர்விற்க்கான நூல் பதிப்பிக்கும் ஒப்பந்தம்.
ஜேப்பி பிரதர்ஸ் என்பது மருத்துவ நூல்களை மட்டுமே பதிப்பிக்கும் நிறுவனம். முதல் வருடம் உடற்கூறியல் (அனாடமி) படிக்கும் இந்தர்பிர் சிங் நூலில் இருந்து, இரண்டாம் வருடம் மருந்தியல் (பார்மக்காலஜி) கே.டி.திரிபாதி, நோய்க்குறியியல் (பதாலஜி) ஹார்ஷ் மோகன் என்று மருத்துவக்கல்லூரியில் பாட நூல்களாக உள்ள பாதி நூல்கள் அவர்கள் நூல்கள் தான். அங்கு நூலை பதிப்பிக்கும் வாய்ப்பு என்பது அந்த காலத்தில் நினைத்து பார்க்கவே முடியாத ஒன்று. அதை விட முக்கியம் அந்த நிறுவனத்தின் சேர்மன் என்னை அலைபேசியில் தொடர்பு கொண்டது. வழக்கமாக அது போன்ற சர்வதேச பதிக்கங்களில் மருத்துவ நூல்களை பதிப்பிக்க வேண்டுமென்றால் முதலில் விண்னப்பிக்க வேண்டும். பிறகு அவர்களின் சென்னை அலுவலகத்தில் இருந்து தொடர்பு கொள்வார்கள். ஒரு படிவத்தை பூர்த்தி செய்து அனுப்பி, பிறகு ஓரிரு அத்தியாயங்களை எல்லாம் அனுப்பி என்று மிகப்பெரிய நடைமுறை உள்ளது. இது எதுவும் இல்லாமல் எனக்கு நேரடியாக வாய்ப்பு கிடைத்தது.
அப்பொழுது நான் மதுரையில் இருந்தேன். மடிக்கணினி எல்லாம் இல்லாத காலம். கணினி இருந்தது வீட்டில். ஆனால் நூல் எழுத வேண்டுமே. தினமும் மருத்துவமனை பணி முடிந்த பிறகு மதுரை மருத்துவக்கல்லூரி நூலகம் சென்று குறிப்புகளை எழுதுவேன். பிறகு மாலை தமிழ்நாடு பொது தேர்வாணையம் (டி.என்.பி.எஸ்.சி) தேர்விற்கு நண்பர்களுடன் படிப்பு. பிறகு சாப்பிட்டு விட்டு குட்டித்தூக்கம். பிறகு 2 மணிக்கு வண்டியை எடுத்து விட்டு, பெரியார் நிலையம் அருகில் இருக்கும் ஒரு இணைய உலாவி கடையில் (அந்த கடை 24 மணி நேரம் திறந்திருக்கும்) 6 மணிவரை அமர்ந்து குறிப்பெடுத்த விபரங்களை அடித்து விட்டு, அதை என் மின்னஞ்சலுக்கு அனுப்பிவிட்டு (அப்பொழுது பென் டிரைவ் கிடையாது) மீண்டும் விடுதி வந்து குளித்து விட்டு வார்டிற்கு சென்று, அறுவை அரங்கிற்கு சென்று, நூலகம் சென்று என்று வாழ்க்கை ஓடிக்கொண்டே இருந்தது.
ஞாயிறு வீட்டிற்கு செல்லும் போது, அந்த வாரம் அடித்த விஷயங்களை எல்லாம் தொகுத்து இப்படியாக ஒரு ஆறு வாரத்தில் நூலை தயார் செய்து அனுப்பினேன். பின்னர் அங்கிருந்து புரூப் ரீடிங் காபி எடிட்டிங் செய்து வந்தது. பிறகு படங்கள். இறுதியாக நூல் வந்தது. வந்தவுடன் விற்றது. அப்பொழுது எல்லாம் கோட்டயம் போன்ற இடங்களில் மாணவர்கள் மொத்தமாக அமர்ந்து படிப்பதால், ஒரு நூல் பிடித்திருந்தால் உடனே அனைவரும் வாங்கி விடுவார்கள்.
தமிழ் நாடு தேர்வாணய தேர்வு முடிந்து நான் அரசு பணியில் சேர்ந்தவுடன், நான் தேர்விற்கு தயார் செய்த குறிப்புகளை தொகுத்து நூலாக வெளியிட்டேன். இன்று வரையில் கிட்டத்தட்ட இரண்டு தசாப்தங்களாக அது தான் நம்பர் ஒன். பிறகு தமிழ்நாடு பட்டமேற்படிப்பு நுழைவுத்தேர்விற்கான நூல் வெளியிட்டேன்
நுழைவுத்தேர்வு நூல்களில் கேள்வி மற்றும் அதற்கான விடை ஏ,பி,சி,டி என்றூ மட்டுமே இருந்த, விடை எந்த நூலில் உள்ளது போன்ற விபரங்கள் இல்லாக ஒரு காலகட்டத்தில் இருந்து, விரிவான விளக்கங்களை மறுமொழிகளில் சுட்டி 1 பாணியில் மாற்றியது தான் நான் பெற்ற வெற்றிகளுக்கு காரணம். அதன் பிறகு தான் மருத்துவ பட்டமேற்படிப்பு நூல்கள் விரிவான விளக்கத்துடன் வந்தன. அடுத்து இது போல் மருத்துவ பாடத்தில் உள்ள விளக்கங்களை எல்லாம் தொகுத்து Pre PG Medical Handbook தொகுத்தேன். அதுவும் தொடர்ந்து அதிக விற்பனையானது. அதை தொடர்ந்து ஒவ்வொரு பாடத்திற்கும் என்று தனியாக நூல்களை பிற மருத்துவர்கள் எழுத ஆரம்பித்தார்கள். இது போல் வந்த நூல்களில் சமீபத்தில் வந்த, மருத்துவர் மாலதி முருகேசன் எழுதிய MICRONS (மறுமொழிகளில் சுட்டி 4 பார்க்கவும்) அருமையாக உள்ளது. தற்சமயம் எம்.பி.பி.எஸ் படிப்பவர்கள் கட்டாயம் வாசிக்கவும் பிறகு ஒவ்வொரு ஊரிலும் வகுப்பு எடுக்க ஆரம்பித்தார்கள், ஆனால் விதை நான் போட்டது (தேவர் மகன் மாடுலேஷனில் வாசித்துக்கொள்ளவும்)
இளம் மருத்துவர்களுக்கான Receptor என்ற பத்திரிகையின் ஆசிரியர் குழுவிலும் இருந்தேன். 2004 ஆண்டே என் வலைத்தளங்களில் நூல்களை விற்க துவங்கிவிட்டேன். மணிஆர்டர், செக் மூலம் பணம் செலுத்தினால் வீட்டிற்கு கூரியர் மூலம் நூல்களை அனுப்பினேன். 2007ல் எனது தளம் இப்படித்தான் இருந்தது. மறுமொழிகளில் சுட்டி 5 பார்க்கவும்
எனது நூல்களில் உள்ள விபரங்களை – அதாவது ஒவ்வொரு கேள்விக்கும் உள்ள பதில்களை – எனது தளங்களில் வெளியிட்டு, யாராவது கூகிளில் அந்த கேள்வியை அல்லது அந்த பதில் குறித்து தேடினால் அவர்கள் என் தளத்திற்கு வந்து அதன் பிறகு அங்கு என் நூலின் விளம்பரத்தை பார்த்து அதை வாங்குவார்கள். இதற்காக 2001 முதல் 2008 வரை கிட்டத்தட்ட 10000 பக்கங்களை சுமார் 25 தளங்களில் உருவாக்கினேன்.
இது தவிர PHPBB மென்பொருள், PHP Nuke மென்பொருளில் சில தளங்களை நடத்தி அங்கு எல்லாம் மருத்துவ மாணவர்கள் விவாதம் செய்ய வழி வகை செய்தேன். யாகூ, கூகிள் மின்னஞ்சல் குழுமங்கள் ஆர்குட் குழுமங்கள் நடத்தினேன். கூகிள் இலவசமாக குறுஞ்செய்தி குழு நடத்த வசதி தந்த போது அதையும் செய்தேன். மறுமொழிகளில் சுட்டி 6 http://labs.google.co.in/smschannels/subscribe/TargetPG பார்க்கவும் இப்படி ஒரு விஷயம் இருந்தது எத்தனை பேருக்கு தெரியும் .
நான் இது வரை நான்கு பதிப்பாளர்களுடன் பணியாற்றியுள்ளேன். யாருமே எனக்கு ராயல்டி தராமல் இருந்ததில்லை. ஏனென்றால் என் நூல்கள் விற்றன பல ஆயிரம் பிரதிகள் வெளிவந்த ஒரே மாதத்தில் விற்றன. இத்தனைக்கும் ஒரு நூலுக்கு கூட நான் வெளியிட்டு விழா நடத்தியதில்லை. எந்த மகாசன்னிதானமும் அங்கிகாரம் தர வேண்டி நின்றதில்லை. ஆனால் மின்னஞ்சல், மின்னஞ்சல் குழுமங்கள், வலைத்தளம், வலைப்பதிவு, ஆர்குட், விவாததளங்கள், குறுஞ்செய்தி குழு, பிறகு முகநூல் குழுக்கள் என்று அனைத்து விதங்களிலும் நூலை அறிமுகப்படுத்தினேன்.
எனது ஒரு நூல் வெளிவருவதற்கு இரு வாரத்திற்கு முன்னர் இருந்து அந்த நூலில் இருந்து சில பக்கங்களை இந்த குழுமங்கள், தளங்கள் என்று வெளியிட்டு வந்து (இன்றைய மொழியில் டீசர்) நூல் வெளியீட்டை அறிவிப்பேன். உடனே விற்று விடும். ஒரு முறை நெல்லை ஈகிள் புக் கடைக்காரர் சொன்னார். அது எப்படி சார், உங்க புக் மட்டும் வந்து இறங்கிய இரண்டாம் நாளை நூறு பேர் ஒரே நாளில் வந்து கேட்கிறார்கள். எப்படி என்று கேட்டார். “ஹிந்துலயும், தினத்தந்தியிலேயே புல் பேஜ் ஆட் சார்” என்று கூறினேன். இதற்கு பின்னால் 40 தளங்களில் உள்ள (வலைத்தளங்கள் உட்பட) 10000க்கும் மேற்பட்ட பக்கங்கள், ஒரு டஜன் யாகூ, கூகிள் குழுமங்கள், அரை டஜன் புல்லட்டின் போர்டுகள், வோர்ட்பிரஸ், PHPBB, PHP Nuke எல்லாம் பயன்படுத்துதால் கனவு கூட SELECT * FROM [targetpg_mcqsonli] WHERE [exam] = “TNPSC”; என்று வருகிறது என்று கூறினால் அவருக்கு புரியுமா
பிறகு சில விஷயங்கள் ஒரே நேரத்தில் நடந்தன
- 1. பிறகு முகநூல் வந்ததால் வளைத்தளங்களும், விவாத தளங்களும், மின்னஞ்சல் குழுமங்களும், குறுஞ்செய்தி குழுமங்களும் காலாவதியாகின.
- 2. மூளை முதுகுத்தண்டு நரம்பியல் அறுவை சிகிச்சை படிப்பில் சேர்ந்து நான் பேனா தூக்கும் நேரம் குறைந்து கத்தி தூக்கும் நேரம் அதிகரித்தது
- 3. திறன்பேசி வந்த பிறகு அச்சு நூல்களின் தாக்கம் குறைந்து பிடிஎப் கோப்புகளின் பயன்பாடு அதிகரித்தது
எனவே எழுத்தாளர் – ஆசிரியர் – தொகுப்பாளர் – போட்டோஷாப் நிபுணர் !! பதிப்பாளர் – இணைய விளம்பர விற்பனையாளர் புருனோ சற்றே பின் சென்றார் 2009ல் பன்றிக்காய்ச்சல் (மறுமொழிகளில் சுட்டி 7) என்ற ஒரு நூல், சில நூல்களின் மறுபதிப்பு தவிர பெரிதாக எதுவும் செய்யவில்லை. எனவே பலரும் பேலியோ எனது முதல் நூல் என்று தவறாக நினைக்கிறார்கள்
2013ல் SCRIBD என்ற இணையதளம் ஒரு சேவையை வழங்கியது. அதாவது உங்கள் நூல்களை ஒருவர் தரவிறக்கம் செய்யாமலேயே அதை அந்த தளத்தின், செயலியில் வாசிக்க உங்களுக்கு பணம் செலுத்தும் வசதி. உடனே எனது சில நூல்களை அதில் ஏற்றினேன். பணம் வந்தது. பிறகு அதே வசதியை சற்று மேம்படுத்தி அமேசான் கிண்டில் டைரக்ட் கொண்டுவந்தது. உடனே எனது சில நூல்களை கிண்டிலில் ஏற்றினேன். முதல் மாதத்தில் 8 டாலர் வந்தது.
10725988 Nov 01, 2013 – Nov 30, 2013 Amazon.com Paid Jan 23, 2014 EFT USD 8.15 62.32 INR 507.88
Sales Period Accrued Royalty Tax Withholding Net Earnings Source
Nov 01, 2013 – Nov 30, 2013 USD 1.40 USD 0.42 USD 0.98 Sales
Nov 01, 2013 – Nov 30, 2013 USD 8.55 USD 2.56 USD 5.99 Sales
Nov 01, 2013 – Nov 30, 2013 USD 1.68 USD 0.50 USD 1.18 Sales
Adjustments USD 0.00
Totals USD 8.15
மாதா மாதம் பணம் வந்து கொண்டே இருந்தது. பிறகு இந்திய ரூபாயில் வர ஆரம்பித்தது
2018ஆம் ஆண்டு போட்டி நடந்த போது தான் எனக்கு போட்டி குறித்து தெரியவந்தது. இதுநாள் வரை நான் கிண்டிலில் எழுதி பதிப்பித்திருந்தவை அனைத்துமே ஆங்கில புத்தகங்கள் மருத்துவத்துறை சார்ந்த புத்தகங்கள். எனவே தமிழ் கிண்டில் நிலவரம் குறித்து அறிந்து கொண்டு அதில் பங்கு பெற அவகாசம் இல்லை. அதனால் 2019ல் பங்கு பெறலாம் என்று முடிவு செய்தேன்.
தமிழ் கிண்டில் நிலவரம் எப்படி என்று பார்க்க எனது மூன்று நூல்களை 2019 பதிப்பித்தேன் – ஒரு சிறுகதை, ஒரு வரலாறு, ஒரு வலைப்பதிவுகளின் தொகுப்பு. இதை வைத்து நான் கற்றுக்கொண்டேன்.
இதை வைத்து என்ன கற்றுக்கொள்ள முடியும் என்று கேட்டால், முதன் முதலில் கிண்டிலில் 3 நூல்கள் வெளியிட்ட ஒருவர் அதிலிருந்து கற்றுக்கொள்ளும் அனுபவத்தை விட 20ஆண்டுகளா நூல்களை எழுதி, தொகுத்து, பதிப்பித்து, இணையம் மூலம் விற்ற என்னால் ஆயிரம் மடங்கு கற்றுக்கொள்ள முடியும்.
அதன் அடிப்படையில் ஆங்கில நூல்களுக்கு வேறு ஆசிரியர் கணக்கு, தமிழ் நூல்களுக்கு வேறு ஆசிரியர் கணக்கு என்று முடிவு செய்தேன். மேலும் இரு தமிழ் நூல்களை கிண்டிலில் போட்டு 2019 நவம்பர் தமிழ் கிண்டில் நிலவரத்தை துல்லியமாக அறிந்து கொண்டேன்.
அதன் படி எனது பேலியோ நூலை மீண்டும் எழுதினேன். போட்டியின் இறுதி நாள் வரை இருக்கும் நிலவரங்களுக்கு ஏற்றாற்போல் சில பல மாற்றங்களை செய்து டிசம்பர் 14ஆம் தேதி காலை வெளியிட்டேன். அன்று இரவு பொதுவில் முகநூலிலும் டிவிட்டரிலும் தெரியப்படுத்தினேன். டிசம்பர் 15ஆம் தேதி மாலையே இது சுட்டி 8 என்ற பிரிவில் அதிகம் விற்பனையாகும் நூல் BESTSELLER என்று வந்து விட்டது. மேலும் இந்திய அளவில் அதிக விற்பனையாகும் நூல்களில் (சுட்டி 9) 8ஆம் இடத்திற்கு வந்து விட்டது. தொடர்ந்து இந்த நூல் 20க்குள் இருந்தது குறிப்பிடத்தக்கது. ஆனால் நான் சும்மா இருந்து நூல் தானாக விற்கவில்லை. நான் தொடர்ந்து வேலை செய்ததால் மட்டுமே என் நூல் விற்றது
டிவிட்டரிலும் முகநூலிலும் அறிமுகப்படுத்திய பிறகு, இரண்டு நாட்கள் கழித்து வாட்சப் சென்றேன். என்னிடம் இருந்த 20000 எண்களுக்கும் தனித்தனியே வாட்சப் அனுப்பினேன். என் நூல் விற்கவில்லை, எனக்கு மதிப்புரை வரவில்லை என்று புகார் செய்யும் யாராவது 20000 பேருக்கு வாட்சப் அனுப்பினீர்களா என்று உங்கள் மனசாட்சியை கேளுங்கள். வாங்குவேன் என்று கூறியவர்களின் எண்களை குறித்துக்கொண்டு அவர்கள் வாங்கும் வரை தொடந்து நினைவூட்டிக்கொண்டிருந்தேன். இப்படியாக 19ஆம் தேதி amazon.com வலைத்தளத்தில் தமிழில் அதிகம் விற்பனையாகும் நூல் என்ற இடத்திற்கு வந்தது
பிறகு இந்திய அமேசனின் தமிழ் பிரிவில் (சுட்டி 10) 3ஆம் இடத்திற்கு வந்து இரண்டாம் இடத்திற்கு வந்து முதலிடத்திற்கு வந்து, 30ஆம் தேதி வரை முதலிடத்தில் இருந்து, ஒரு நாள் மட்டும் கிழிறங்கி, மீண்டும் 31ஆம் தேதி முதலிடத்திற்கு வந்தது ஜனவரி 13ஆம் தேதி வரை முதலிடத்தில் இருந்தது. (அந்த ஒரு நாள் மட்டும் கீழிறங்கியதற்கு காரணம் என்னவென்று கிழே விளக்கியுள்ளேன்.)
வாட்சப் முடிந்த பிற்கு டெலிகிராம். அதன் பிறகு முகநூல் என்று தொடர்ந்து அனைவருக்கும் தெரியப்படுத்திக்கொண்டே இருந்தேன். அதனால் தான் நூல் விற்பனையில் தொடர்ந்து முதலிடம் இருந்தது
நான் எதிர்பார்த்த எண்ணிக்கை விற்ற பிறகு இரண்டு நாட்கள் இலவசமாக அளித்து மின்னஞ்சல் கூழுமங்கள், முகநூல் குழுமங்கள் ஆகியவற்றில் தெரியப்படுத்தினேன். நான் எழுதிய குழுமங்களில் இருக்கும் உறுப்பினர்கள் மொத்தம் 20 லட்சத்தை தாண்டும். எனவே நான் எதிர்பார்த்த எண்ணிக்கையில் நூல்கள் இலவசமாக விற்றன. இலவசம் அளித்த போது ஒரு நாள் மட்டும் தான் பேலியோ நூல் முதலிடத்திலிருந்து (சுட்டி 10ல்) இறங்கியது.
போட்டியின் கடைசி நாளன்று புத்தகம் வெளியிட்டு இரண்டே வாரங்களில் புருனோ எப்படி முதல் கட்டத்தில் வென்றார் என்ற பலரும் கேட்கிறார்கள். உண்மையில் நான் எப்படி வென்றேன் என்று அறிய விரும்பினால், என்னிடம் நேரடியாக கேட்டால் பாடம் நடத்தியிருப்பேன். ஆனால் அந்த கேள்வியை கேட்கும் நபர்களின் நோக்கம், அறிவுத்தாகம் அல்ல, நக்கல் மட்டுமே. அதனால் தான் என்னிடம் கேட்காமல், மற்றவர்களிடம் கேட்கிறார்கள். நூலக ஆர்டரால் ஆயிரம் பிரதிகள் அச்சுநூல்கள் மட்டுமே எழுதியவர்களும், விற்பவர்களும், முதன் முதலில் கிண்டிலில் எழுதியவர்களும், இதை எனது முதல் நூலாக, எனது முதல் கிண்டில் முயற்சியாக நினைத்து அறியாமையால் இந்த நக்கல் கேள்வியை முன்வைக்கிறார்கள்.
உண்மையில் அவர்கள் கேட்க வேண்டிய கேள்வி, பிரபலமான தமிழ் புத்தகங்கள் பட்டியலில் தொடர்ந்து மூன்று வாரங்கள் புருனோவின் நூல் எப்படி முதலிடத்தில் இருந்தது என்பதுதான். காரணம் அப்படி முதலிடத்தில் இருந்ததால் தான் இந்த நூல் அடுத்த கட்டத்திற்கு தேர்வானது. எந்த நூல் விற்பனையில் முதலிடத்தில் இருந்துள்ளது என்பதை இவர்கள் கவனிக்கவில்லை என்பதால் தான் இந்த கேள்வியே என்பது வேறு விஷயம்
நண்பர்கள் ரவியோ, சென்னோ இல்லாமல் இந்த இடம் சாத்தியமில்லை என்பதை அழுத்தமாக பதிவு செய்கிறேன். ஆனால் ரவியும் சென்னும் எனக்கு எவ்வளவு உதவினார்களோ, அதே அளவு மற்றவர்களுக்கும் உதவினார்கள் என்பதை என்னால் கண்டிப்பாக கூற முடியும். ஒவ்வொரு நூலும் வெவ்வேறு அளவு விற்றதற்கு காரணம் அவர்களின் பாரபட்சம் அல்ல. அந்த அந்த நூலாசிரியரின் பிற நூல்கள் மற்றும் இந்த நூல் மற்றும் அவர்கள் சந்தைப்படுத்திய விதம் தான்.
தமிழ் இலக்கிய உலகில் நூல் விற்க
1. யாரவது இலக்கிய பீடம் முன்னுரை எழுத வேண்டும்
2. பணம் செலவழித்து வெளியீட்டு விழா நடத்த வேண்டும். விழா நடந்த பிறகு மதுவிருந்து வேறு தனியாக நடத்த வேண்டும்
3. புரிந்தும் புரியாமலும் இருக்கும் மொழியில் அந்த நூலிற்கு விமர்சனம் வேண்டும்
4. நூலகங்கள் அந்த நூலை வாங்க வேண்டும்
ஆனால் என் பாணி என்பது வேறு. சொல்லப்போனால் மேலே கூறிய நான்கு விஷயங்களை தவிர மீதி முறைகளில் தான் நான் கவனம் செலுத்தினேன்
இந்த அளவு விற்பனை, இந்த (மூன்று வாரங்கள்) தொடர் முதலிடம் என்பது தற்செயல் அல்ல. அதிர்ஷ்டம் உள்ளது. ஆனால் அதிர்ஷ்டம் மட்டும் காரணம் அல்ல. இதற்கு பின்னால் மின்னஞ்சல் குழுமங்கள், முகநூல் குழுமங்கள் (குழும நிர்வாகிகளுக்கு நன்றிகள்), எந்த மென்பொருள் உதவியும் இல்லாமல் நான் அனுப்பிய 20000 வாட்சப் செய்திகள் என்று பலவும் உள்ளன. டிசம்பர் 14 முதல் ஜனவரி 1 வரை தொடர்ந்து ஓடிக்கொண்டே இருந்தேன். ஆனால் எனது செயல்பாடுகள் என்பது முற்றிலும் வெவ்வேறு தளங்களில் இருந்ததால் அது பலரது கவனத்தில் இல்லை. எனவே அவர்கள் எல்லாம் நான் எதுவும் செய்யாமலே நான் வென்றதாக நினைக்கிறார்கள்
-oOo-
சுய புராணம் போதும், அடுத்து என்ன என்று கேட்கிறீர்களா ?
முகநூலும், யூடுயுபும் எப்படி உங்களின் சிந்தனையை தாக்குகின்றன என்றும், ஒரு கருத்துடன் முகநூலில் / யூடுயுபில் நுழையும் நீங்கள் எப்படி அந்த கருத்தில் உறுதியாகிறீர்கள் (அது தவறாக இருந்தாலும் கூட) என்றும், இதனால் தற்காலத்தில் பசி, பட்டினி, நோய்கள், மரணம் அதிகரிப்பது எப்படி என்றும், இதனால் மனித குலத்திற்கு நீண்ட நாட்களில் ஏற்படும் நன்மை என்ன என்பது குறித்தும் 10 பக்கங்களில் ஒரு சிறுகதை எழுதியுள்ளேன்
தமிழில் : ஆர்கானிக் யூஜெனிக்ஸ் : செயற்கை நுண்ணறிவும் இயற்கை மூடத்தனமும் (மறுமொழிகளில் சுட்டி 11)
ஆங்கிலத்தில் : Artificial Intelligence and Natural Stupidity: Organic Eugenics (மறுமொழிகளில் சுட்டி 12)
கதையை வாசித்து உங்கள் கருத்துக்களை பகிருங்கள்
எனது அனைத்து நூல்களும் மறுமொழிகளில் சுட்டி 13ல் உள்ளன
வெற்றி பெற்ற பேலியோ நூலை வாங்க மறுமொழிகளில் சுட்டி 14 செல்லவும்
ஒரு முறை ஒரு பிரபல பாடகருடன் பேசிக்கொண்டிருந்தோம். அப்பொழுது ஒருவர் அந்த பாடகரிடம் “நான் உங்கள் பாடல்களை எல்லாம் தினமும் கேட்கிறேன். எனக்கு உங்களை போல் பாடகராக வேண்டும் என்பதே லட்சியம்” என்று கூறினார். பாடகரும் பெருந்தன்மையுடன் “நல்லது தம்பி” என்று கூறினார். நான் குறுக்கே புகுந்து, “பிரதர், நீங்க சார் மாதிரி ஆகவேண்டுமென்றால் சார் பாடிய பாடல்களை மற்றும் கேட்டால் போதாது. சார் 10 வயதில் இருந்து என்ன செய்தார், எப்படி பயிற்சி செய்தார், என்னவெல்லாம் கற்றார் என்று பாருங்கள். சச்சின் மேட்சில் ஆடுவதை பார்த்தால் சச்சின் ஆகவே முடியாது. சச்சின் நெட் பிராக்டிசில் என்ன செய்கிறார் என்று பார்க்கவேண்டும்” என்று கூறினேன். பாடகர் என்னை சில நொடிகள் கூர்ந்து பார்த்தார். பிறகு புன்முறுவல் வந்தது. “ரொம்ப சிம்பிளா முடிச்சிட்டீங்க தம்பி” என்றார்.
உசேன் போல்ட் தங்கப்பதக்கம் வாங்குவது அவரது 10 நொடி ஓட்டத்திற்காக மட்டுமல்ல. அந்த பத்து நொடிகளும் ஒழுங்காக ஓட வேண்டும். அது அவசியம். ஆனால் அது மட்டும் போதாது. அந்த பத்து நொடிகளுக்கு பின்னால் இருக்கும் பல வருட தயாரிப்புகளுக்காத்தான் அந்த பதக்கம். அதே போல், பேலியோ நூல் தொடர்ந்து மூன்று வாரங்கள் விற்பனையில் முதலிடம் பெற்றது என்றால் அது இந்த நூலின் தரம், மற்றும் எனது இரு வார செயல்பாடுகளால் மட்டுமல்ல். நான் 20 ஆண்டுகளாக எழுதிய நூல்கள், நான் என் தளங்கள் மூலம் விற்ற 100க்கும் மேற்பட்ட நூல்கள், சுமார் 20 வருடங்களாக என்னை தொடர்ந்து வாசிக்கும் பல ஆயிரம் நண்பர்கள், கிண்டிலில் மட்டுமே 6 வருட அனுபவம், போன்ற பல காரணங்கள் உள்ளன.
நான் இதையெல்லாம் எழுதுவது என்னை நக்கலடித்தவர்களுக்காக அல்ல. உண்மையில் இதை அறிந்து கொள்ள ஆர்வத்துடன் இருந்து, ஆனால் கேட்க தயக்கத்துடன் இருக்கும் பலருக்காக
audentes Fortuna adiuvat, Fortune favours the brave என்ற கூற்றின் படி வேலை செய்தால் அதிர்ஷ்டம் வரும். வெற்றிக்கு காரணம் 1 சதம் அறிவு, 99 சதம் உழைப்பு. Genius is one percent inspiration and ninety nine percent perspiration



 1. அந்த துறை குறித்த பொதுவான அடிப்படை அறிவு
1. அந்த துறை குறித்த பொதுவான அடிப்படை அறிவு
 Imagine two scenarios
Imagine two scenarios
 The pharmacist, who had to PREPARE THE DRUG, had to be very careful. Adding 5gm of a substance when 5 mg has to be added would be fatal. Hence Pharmacy was a specialist discipline and A Pharmacist was needed for each and every medical shop. That was the time such regulations were made. Only in that backdrop, it was made that a Pharmacy needs a Pharmacist
The pharmacist, who had to PREPARE THE DRUG, had to be very careful. Adding 5gm of a substance when 5 mg has to be added would be fatal. Hence Pharmacy was a specialist discipline and A Pharmacist was needed for each and every medical shop. That was the time such regulations were made. Only in that backdrop, it was made that a Pharmacy needs a Pharmacist Medicine has been evolving. Disciplines like Grief counselling, Nutrition, Diet, Transplant Co ordinator etc are coming up
Medicine has been evolving. Disciplines like Grief counselling, Nutrition, Diet, Transplant Co ordinator etc are coming up That is really appreciable. But at the same time, we need to also educate the police and in case the patient requires surgery, it is better to keep the stomach free of any fluids. Of course, accident victims will feel thirst due to two mechanism (1) Blood Loss –> Hypovolemia (2) Sympathetic System Surge –> Dry Mouth , but don’t give anything by mouth till treatment plan is finalised
That is really appreciable. But at the same time, we need to also educate the police and in case the patient requires surgery, it is better to keep the stomach free of any fluids. Of course, accident victims will feel thirst due to two mechanism (1) Blood Loss –> Hypovolemia (2) Sympathetic System Surge –> Dry Mouth , but don’t give anything by mouth till treatment plan is finalised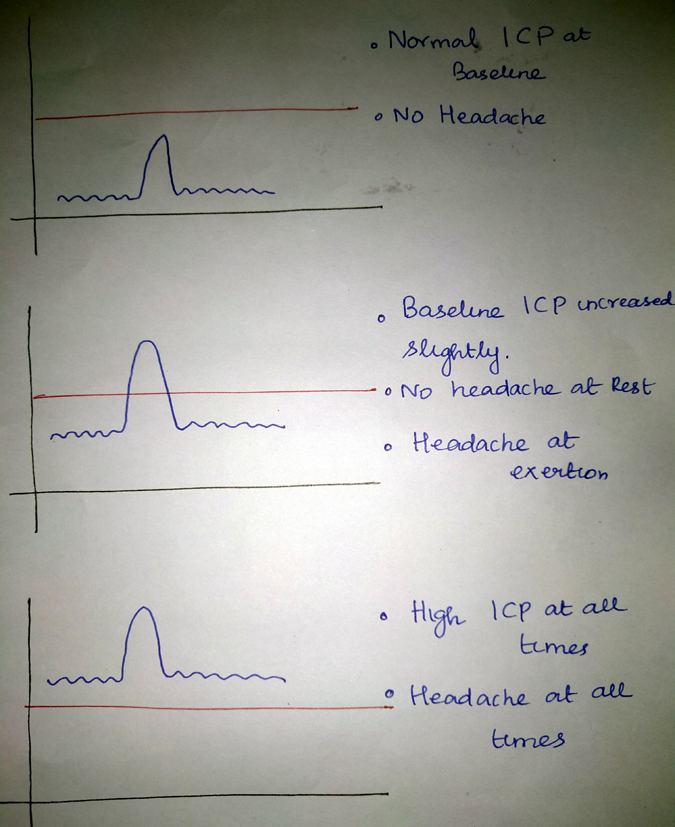

 I did an Clinical Examination and as expected the Fundus (Eye) showed early eigns of increased pressure inside the skull. It can be any infection or tumour. MRI of Brain Revealed Infection of the coverings of the brain with Tuberculous bacteria. The patient took proper treatment and the infection has been cured and the pressure has come back to normal and when you see the Eye (Fundus) now, there is no sign of raised pressure
I did an Clinical Examination and as expected the Fundus (Eye) showed early eigns of increased pressure inside the skull. It can be any infection or tumour. MRI of Brain Revealed Infection of the coverings of the brain with Tuberculous bacteria. The patient took proper treatment and the infection has been cured and the pressure has come back to normal and when you see the Eye (Fundus) now, there is no sign of raised pressure
 Shopping means getting possession of a new article
Shopping means getting possession of a new article